Well, see for you self...
But seriously, listen to this interview for a viewpoint of a real patient privacy advocate, Deborah C. Peel MD,MD. Also, see their website.
Wednesday, October 31, 2007
Another HIE related failure
Just read in Modern Health , "Patient Safety Institute folds due to lack of funding".
Unfortunately this is another case of an HIE or RHIO living off grants only to find out later that there's no true sustainability model to keep it going after the initial grant funding dries up. No one felt there was enough value in the HIE to justify further investment.
With many HIEs, its always easy to use someone else's money (i.e, government funding) to get things started. These efforts always begin with high hopes of all kinds of benefits to patient safety, cost reduction, greater efficiency etc. Somehow, when its time to use your own money, these benefits don't seem worth it. My feeling is that many of these HIEs are set up as huge bureaucracies, with all the "C's"- CEOs, COOs, CIOs. There really is no way an HIE can support this type of boated infrastructure. HIEs really need to be "lean" in order to succeed.
Unfortunately this is another case of an HIE or RHIO living off grants only to find out later that there's no true sustainability model to keep it going after the initial grant funding dries up. No one felt there was enough value in the HIE to justify further investment.
With many HIEs, its always easy to use someone else's money (i.e, government funding) to get things started. These efforts always begin with high hopes of all kinds of benefits to patient safety, cost reduction, greater efficiency etc. Somehow, when its time to use your own money, these benefits don't seem worth it. My feeling is that many of these HIEs are set up as huge bureaucracies, with all the "C's"- CEOs, COOs, CIOs. There really is no way an HIE can support this type of boated infrastructure. HIEs really need to be "lean" in order to succeed.
Friday, October 26, 2007
Healthcare Business Intelligence
I just read that FierceHealthIT listed Qlik Tech as its top 3 HealthIT innovator. Many are familiar with companies like Cognos, Business Objects and Microsoft, but this company is really hot. Its big selling point is its "In Memory Analytics" which allows it to perform ultra-fast "what-if" analyses on hugh datasets.
What I like about this company's approach is that they allow you to download a trial version of the software. I downloaded the trial version a few weeks ago and must admit it was very easy to get things up and running. I hope to spend a little more time with the trial software later. I am curious however to know the cost to license the software.
What I like about this company's approach is that they allow you to download a trial version of the software. I downloaded the trial version a few weeks ago and must admit it was very easy to get things up and running. I hope to spend a little more time with the trial software later. I am curious however to know the cost to license the software.
PriMed East Boston follow-up
PriMed in Boston this year came and went (see my previous post). Since the conference moved from the Hyne's center in the heart of Boston, near Copley and the Prudential Plaza, to the new convention center on the waterfront, it has become less exciting each year. In the past there was always a vast collection of vendors, especially EMR vendors. This year however, I felt there was barely a handful. Notably absent was eClinicalworks . It also seemed that the physician attendance was also considerably lower.
The Hynes site was much move vibrant due to its presence in the Boston. The new convention center in contrast seems to be in the middle of nowhere, tucked in the midst of warehouses and other industrial buildings. I do hope PriMed organizers take notice and return the conference to the Hyne's.
The Hynes site was much move vibrant due to its presence in the Boston. The new convention center in contrast seems to be in the middle of nowhere, tucked in the midst of warehouses and other industrial buildings. I do hope PriMed organizers take notice and return the conference to the Hyne's.
Thursday, October 11, 2007
Open Source EMR
I just came across some information on an open source EMR on the EMR Update site. The website is located here. Looks fairly interesting. There are a set of very basic screen shots which gives an idea to the look and feel, but also explains the thought process behind the user interface design.
The design of the UI is based on the classic MVC pattern or the Model-View-Controller design pattern. If you're interested in how to implement the MVC pattern in .NET, look at this.
There is an architecture document, but is seems a bit sparse. It does at least show the organization for the project.
The best part is the data model, which is provides a fair amount of detail. It follows a fairly classic healthcare data model for "Patients", "Orders", "Medications" and "Laboratory" entities.
All in all, it looks like fairly neat project. We need more such open source efforts to make the adoption of health IT more affordable. I hope more independent and highly motivated developers take the plunge and really do for Healthcare IT what they did for personal computers and software in the 1980, and the Internet in the 1990's. We can't allow Healthcare IT to be monopolized by the big companies.
The design of the UI is based on the classic MVC pattern or the Model-View-Controller design pattern. If you're interested in how to implement the MVC pattern in .NET, look at this.
There is an architecture document, but is seems a bit sparse. It does at least show the organization for the project.
The best part is the data model, which is provides a fair amount of detail. It follows a fairly classic healthcare data model for "Patients", "Orders", "Medications" and "Laboratory" entities.
All in all, it looks like fairly neat project. We need more such open source efforts to make the adoption of health IT more affordable. I hope more independent and highly motivated developers take the plunge and really do for Healthcare IT what they did for personal computers and software in the 1980, and the Internet in the 1990's. We can't allow Healthcare IT to be monopolized by the big companies.
PriMed East Tomorrow
I'll be attending PriMed East, one of the largest physician trade shows/conference, tomorrow in Boston. Its usually a great place to catch up with people I've known in medicine through the years, in training and in practice. A highlight of the event is the EMR vendors exhibits, where there's always a very broad representation of vendors. If you're an up and coming EMR or Healthcare IT vendor, this is a great place to showcase your product to regular practicing physicians, the ones that really drive healthcare.
I'll be sure to give a run down of the event next week...
I'll be sure to give a run down of the event next week...
Wednesday, October 10, 2007
HL7 v3, A Challenge in Implementation
Its been a while since I've written a technical blog entry. HL7 is a favorite topic of mine, especially HL7 v3. Therefore, after reading David Li's piece in NeoTool's blog, Preparing for HL7 V3, I was motivated to give my 2 cents on the topic.
I've spent a lot of time trying to implement a practical HL7 v3 solution. I quickly realized that to use it for messaging would be highly impractical. There are just too many possible interpretations of how to convey a message using the v3 messaging model. A great quote I remember describing HL7 v3's XML structure, was "they used every trick in the book".
What I did find helpful however was the RIM (Reference Information Model) as a health-care data model. Having said that, I would caution against using the HL7 v3 RIM to model a logical relational database design.
RIM can serve as a very useful starting point for a design, but do not use it too literally. Doing so can lead to a very inefficient and needlessly complex database design. As I learned in engineering school, learning where to make trade-offs is the difference between a practical design and an exact, but impractical design.
I've spent a lot of time trying to implement a practical HL7 v3 solution. I quickly realized that to use it for messaging would be highly impractical. There are just too many possible interpretations of how to convey a message using the v3 messaging model. A great quote I remember describing HL7 v3's XML structure, was "they used every trick in the book".
What I did find helpful however was the RIM (Reference Information Model) as a health-care data model. Having said that, I would caution against using the HL7 v3 RIM to model a logical relational database design.
RIM can serve as a very useful starting point for a design, but do not use it too literally. Doing so can lead to a very inefficient and needlessly complex database design. As I learned in engineering school, learning where to make trade-offs is the difference between a practical design and an exact, but impractical design.
Monday, October 8, 2007
Nursing Homes finally getting attention
FierceHealthIT had an interesting commentary piece on IT in the long-term care setting. As a physician who cares for patients in a nursing home, I know first hand, that caring for a patient in a nursing home is extremely challenging.
There is a complete lack of any IT at most nursing homes. Patients frequently come from multiple sources, such as community and tertiary hospitals. Patients bring with them stashes of paper-- labs, radiology reports, discharge summaries etc. Trying to put all the information together to get a complete view of a patient is nearly next to impossible. It is at the nursing homes where IT- RHIOs/HIEs and telemedicine can have a real impact in the quality of care of patients.
I'm happy to see long-term care finally get some attention.
There is a complete lack of any IT at most nursing homes. Patients frequently come from multiple sources, such as community and tertiary hospitals. Patients bring with them stashes of paper-- labs, radiology reports, discharge summaries etc. Trying to put all the information together to get a complete view of a patient is nearly next to impossible. It is at the nursing homes where IT- RHIOs/HIEs and telemedicine can have a real impact in the quality of care of patients.
I'm happy to see long-term care finally get some attention.
Likely PHR users
HealthVault has really stimulated great discussion on the issue of PHRs. A good part of the discussion is on the viability of the PHR concept and if PHRs concept will really "take off".
The vast number of PHR users are likely going to be the "worried well" (hypochondriacs) or those people with chronic illness who like to track (or in some cases, obsess) over their health issues.
The elderly, who probably would have the most to gain from a PHR for its ability to track long medication lists, multiple doctor visits and hospitalizations, are the same people who would be less likely to use a PHR. And this is not just because the elderly are not computer literate, but because of the usual age related health problems, such as low vision, early dementia etc. We will need to depend on the care givers to manage their PHRs.
To most people however, healthcare is something they hire someone else to worry about (the doctor) in much the same way we have a fund manager to manage our mutual funds. I suspect that it will be the “Quicken” types who will make up the vast majority of PHR users.
The vast number of PHR users are likely going to be the "worried well" (hypochondriacs) or those people with chronic illness who like to track (or in some cases, obsess) over their health issues.
The elderly, who probably would have the most to gain from a PHR for its ability to track long medication lists, multiple doctor visits and hospitalizations, are the same people who would be less likely to use a PHR. And this is not just because the elderly are not computer literate, but because of the usual age related health problems, such as low vision, early dementia etc. We will need to depend on the care givers to manage their PHRs.
To most people however, healthcare is something they hire someone else to worry about (the doctor) in much the same way we have a fund manager to manage our mutual funds. I suspect that it will be the “Quicken” types who will make up the vast majority of PHR users.
Sunday, October 7, 2007
Obstacles for PHRs, HealthVault?
From the WSJ article Microsoft's Health Push Faces Obstacles :
" "Consumers are just not that excited about these" services, said Elizabeth Boehm, an analyst at Forrester Research Inc"
"Few households watch their health closely, so they aren't looking for new health tools. "In general they're not tracking it and don't understand the value of having it equally shareable" in digital form, Forrester's Ms. Boehm said. "They just don't understand what's in it for them.""
I must say that I do agree that most patients are not interested in this detailed level of their healthcare. The PHRs are being promoted/marketed to the general population, while products such as EMRs (electronic medical records) are targeted at a smaller group, the physicians. If just 10% of the population adopts PHRs, this may be considered a success from a consumer business standpoint, but will not necessarily revolutionize how healthcare is practiced. Wide-spread physician adoption is still the key to any healthcare revolution.
Unfortunately, those that consume much of the healthcare resources, the elderly and less affluent, may be less likely to use a PHR. Most PHR users likely will be among the better educated and many of these people will be the so called "worry-wells" (patients that are actually health but worry about their own health disproportionately)
" "Consumers are just not that excited about these" services, said Elizabeth Boehm, an analyst at Forrester Research Inc"
"Few households watch their health closely, so they aren't looking for new health tools. "In general they're not tracking it and don't understand the value of having it equally shareable" in digital form, Forrester's Ms. Boehm said. "They just don't understand what's in it for them.""
I must say that I do agree that most patients are not interested in this detailed level of their healthcare. The PHRs are being promoted/marketed to the general population, while products such as EMRs (electronic medical records) are targeted at a smaller group, the physicians. If just 10% of the population adopts PHRs, this may be considered a success from a consumer business standpoint, but will not necessarily revolutionize how healthcare is practiced. Wide-spread physician adoption is still the key to any healthcare revolution.
Unfortunately, those that consume much of the healthcare resources, the elderly and less affluent, may be less likely to use a PHR. Most PHR users likely will be among the better educated and many of these people will be the so called "worry-wells" (patients that are actually health but worry about their own health disproportionately)
Saturday, October 6, 2007
Microsoft HealthVault for storing our data, Issues regarding Privacy and Security
Many are asking, how secure will my data be? Will hackers be able to access it. Well, who knows? Many of us do online banking, and have trust in this process. With my back account, I know every crook around the word would see me as a target. Money has universal value. With my healthcare data however, I doubt someone on the other side of the world would be interested.
The only people that really might have an interest in my health data would be my family, friends, neighbors or co-workers. One can argue that my employer may as well. The real fear however would be if the government or insurance companies get access to my PHR data. If thats the case, they would not do it illegally by hacking (as would a neighbor). I'm afraid this would only happen if we allow a shift in public policy to take place which would permit our PHR data to be accessed by these other entities.
Once there is a sizable PHR database based on our nations population, it will be too tempting for politicians and policy makers not to try to make arguements to justify use of this data for the "public good". As politicians frequently do, they'll say, "we're doing it for the children".
This is the real threat to the privacy of our data.
The only people that really might have an interest in my health data would be my family, friends, neighbors or co-workers. One can argue that my employer may as well. The real fear however would be if the government or insurance companies get access to my PHR data. If thats the case, they would not do it illegally by hacking (as would a neighbor). I'm afraid this would only happen if we allow a shift in public policy to take place which would permit our PHR data to be accessed by these other entities.
Once there is a sizable PHR database based on our nations population, it will be too tempting for politicians and policy makers not to try to make arguements to justify use of this data for the "public good". As politicians frequently do, they'll say, "we're doing it for the children".
This is the real threat to the privacy of our data.
Google's PHR
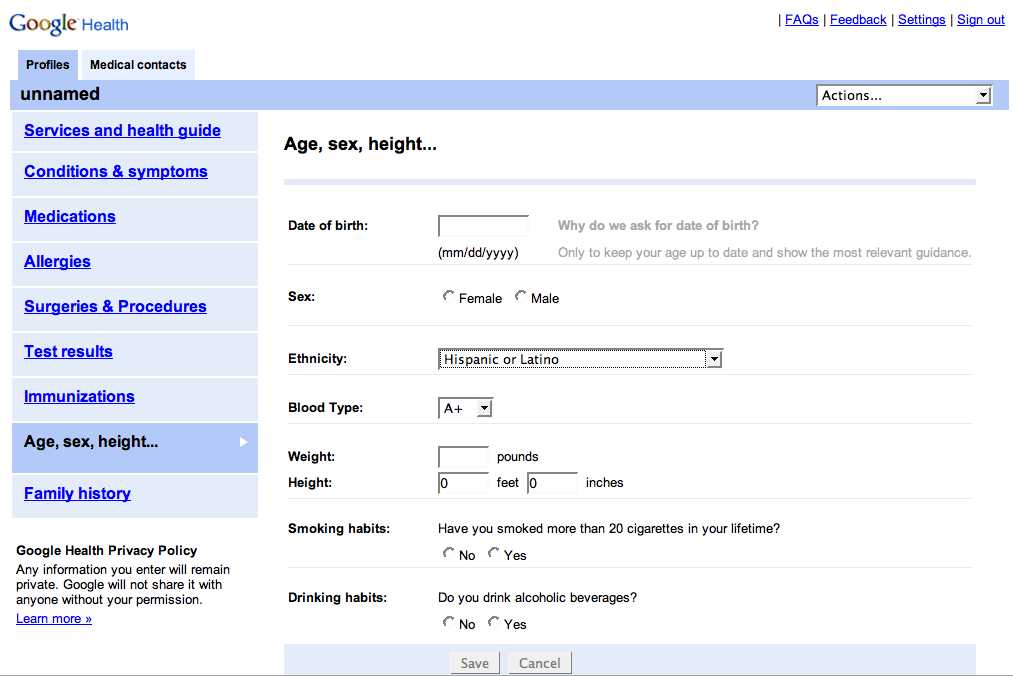 While on the topic of HealthVault and PHRs, the discussion would not be complete without mentioning Google. Here is a link to some screen shots of Google's prototype PHR. This is more of a PHR than Microsoft's Healthvault. My patients and fellow physician colleagues would not have a problem understanding this type of application, its functionality is very obvious. Google's prototype PHR appears to be an "end-product" rather than a set of services like HealthVault.
While on the topic of HealthVault and PHRs, the discussion would not be complete without mentioning Google. Here is a link to some screen shots of Google's prototype PHR. This is more of a PHR than Microsoft's Healthvault. My patients and fellow physician colleagues would not have a problem understanding this type of application, its functionality is very obvious. Google's prototype PHR appears to be an "end-product" rather than a set of services like HealthVault.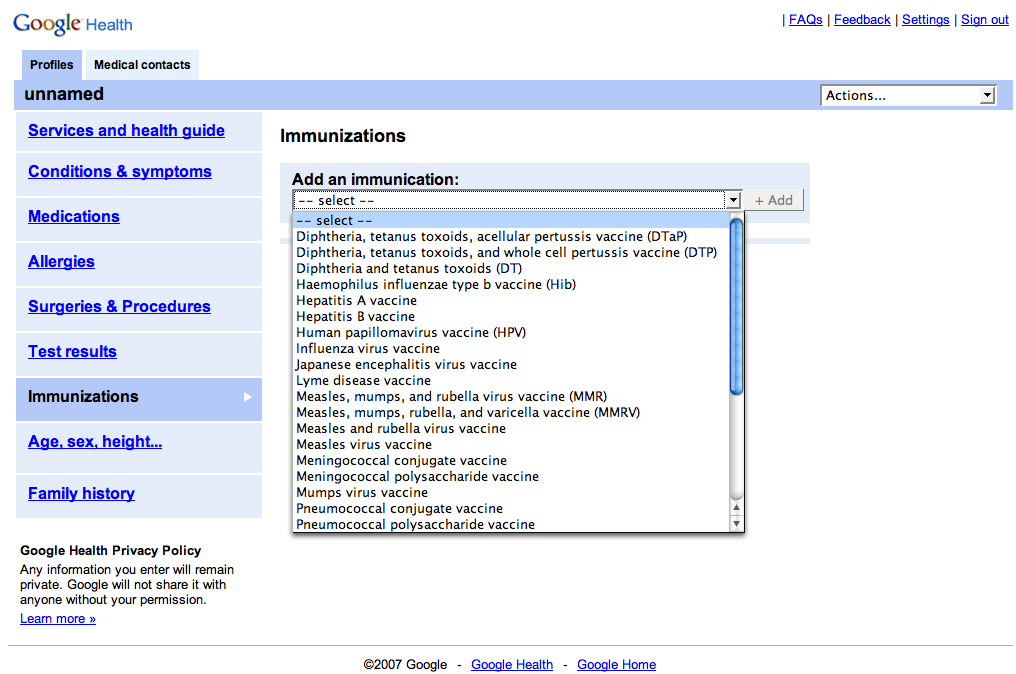

Part III: Understanding how to Develop Applications with HealthVault
Microsoft's HealthVault is not a "PHR" but rather a "PHR platform" with a set of back-end services for secure storage, retrieval and sharing of healthcare information. These services can be used by a developer to actually build what we may describe as a "classic PHR".
What does HealtVautlt mean to me as a developer? How does it work?
Here is the scenario as I see it, which explains how a developer may start to think of ways to use HealthVault:
Developing with HealthVault
- Lets assume a patient, John Doe registers for a HealthVault account. This is where his healthcare data would be stored. John Doe controls access to this data using his "Windows Live ID" credentials (user-name and password).
- Now suppose, I as a developer create a new PHR product called "Acme PHR" using HealthVault on the backend. That is, I develop the presentation layer, the actual website with my company's logo etc. I decide the look and feel of the application and the type of data I want want to collect and store for a patient. Additionally, I would also develop the business layer containing the business rules, knowledge-base and decision support functionality.
The final Acme PHR product is my company's application. The application performs the functions that I want it to perform. I can do interesting things with the application by combining the data in HealthVault with additional data that I define and store separately on my own server/database.
Designing a new HealthVault-based application- Personal Diet Planner and PHR
What do I mean by combining HealthVault data with my own defined data? Lets take an example. Suppose I want my PHR application to have the ability to provide different diets for patients with various health conditions, like diabetes, hypertension or obesity.
With my PHR, I will want to collect patient data such as weight, blood pressure, health conditions, blood sugar values, cholesterol results etc. This data is patient specific, so I decide to use HealthVault as the storage mechanism. Besides the convenience of using HealthVault's APIs, the big advantage of HealthVault is that it handles all the security issues, such as authorization and role based access to data (specified by the patient).
The database of the different diet plans however is stored on my company's servers. It is my company's proprietary data and would be kept entirely separate from HealthVault's data.
With my application, I can combine patient specific data from HealthVault, with my database of diet plans. So if a patient using my PHR, has high blood pressure and is obese, I may recommend a particular diet plan, while someone with just mild obesity, may get another diet recommendation. This is my application's "secret sauce", the ability to decide the proper diet for specific health conditions.
This is an important point, because my application is not about the details of storage and retrieval of health data, but rather, on how I use this patient's specific data and combine it with other data to create new innovative personal healthcare applications. This is much like an operating system. HealthVault essentially acts as an operating system like Windows, handling all the low level detail and chores, while my application focuses on the big picture.
Whats next? More Applications using common HealthVault Data
So patient John Doe uses my "Acme PHR" (with the special diet plan feature), and has entered his health data. John Doe is very happy with my PHR product.
But now, another company creates another product using HealthVault which recommends exercise plans for patients with specific health conditions. John Doe likes this idea. He has all his data already entered via my PHR product and is happy with the diet plan. He now wants exercise recommendations. John Doe can subscribe to this new "Exercise Planner" application. Fortunately, because it too uses HealthVault, John's data is already entered. This data can now be used by this new application. So using John Doe's existing weight, blood pressure and health condition data, an exercise plan can be recommended by this new product. There can be other products which do other things. The possibilities are endless.
HealthVault is like an Operating System
You can see the tremendous advantage of having personal health data stored once, with the ability to use it in multiple ways with disparate products. Just as the Windows operating system has resulted in countless software products, HealthVault likewise may lead to countless health care applications.
What does HealtVautlt mean to me as a developer? How does it work?
Here is the scenario as I see it, which explains how a developer may start to think of ways to use HealthVault:
Developing with HealthVault
- Lets assume a patient, John Doe registers for a HealthVault account. This is where his healthcare data would be stored. John Doe controls access to this data using his "Windows Live ID" credentials (user-name and password).
- Now suppose, I as a developer create a new PHR product called "Acme PHR" using HealthVault on the backend. That is, I develop the presentation layer, the actual website with my company's logo etc. I decide the look and feel of the application and the type of data I want want to collect and store for a patient. Additionally, I would also develop the business layer containing the business rules, knowledge-base and decision support functionality.
The final Acme PHR product is my company's application. The application performs the functions that I want it to perform. I can do interesting things with the application by combining the data in HealthVault with additional data that I define and store separately on my own server/database.
Designing a new HealthVault-based application- Personal Diet Planner and PHR
What do I mean by combining HealthVault data with my own defined data? Lets take an example. Suppose I want my PHR application to have the ability to provide different diets for patients with various health conditions, like diabetes, hypertension or obesity.
With my PHR, I will want to collect patient data such as weight, blood pressure, health conditions, blood sugar values, cholesterol results etc. This data is patient specific, so I decide to use HealthVault as the storage mechanism. Besides the convenience of using HealthVault's APIs, the big advantage of HealthVault is that it handles all the security issues, such as authorization and role based access to data (specified by the patient).
The database of the different diet plans however is stored on my company's servers. It is my company's proprietary data and would be kept entirely separate from HealthVault's data.
With my application, I can combine patient specific data from HealthVault, with my database of diet plans. So if a patient using my PHR, has high blood pressure and is obese, I may recommend a particular diet plan, while someone with just mild obesity, may get another diet recommendation. This is my application's "secret sauce", the ability to decide the proper diet for specific health conditions.
This is an important point, because my application is not about the details of storage and retrieval of health data, but rather, on how I use this patient's specific data and combine it with other data to create new innovative personal healthcare applications. This is much like an operating system. HealthVault essentially acts as an operating system like Windows, handling all the low level detail and chores, while my application focuses on the big picture.
Whats next? More Applications using common HealthVault Data
So patient John Doe uses my "Acme PHR" (with the special diet plan feature), and has entered his health data. John Doe is very happy with my PHR product.
But now, another company creates another product using HealthVault which recommends exercise plans for patients with specific health conditions. John Doe likes this idea. He has all his data already entered via my PHR product and is happy with the diet plan. He now wants exercise recommendations. John Doe can subscribe to this new "Exercise Planner" application. Fortunately, because it too uses HealthVault, John's data is already entered. This data can now be used by this new application. So using John Doe's existing weight, blood pressure and health condition data, an exercise plan can be recommended by this new product. There can be other products which do other things. The possibilities are endless.
HealthVault is like an Operating System
You can see the tremendous advantage of having personal health data stored once, with the ability to use it in multiple ways with disparate products. Just as the Windows operating system has resulted in countless software products, HealthVault likewise may lead to countless health care applications.
Friday, October 5, 2007
PHRs, too much Hype?
HIStalk's comments on HealthVault were very insightful as usual. I think the industry is a little too high on the concept of PHR. As HISTalk hinted, I do doubt most patients want to manage the details of their own health records. Much the same way that most of us would rather have Fidelity manage our 401Ks than having to try controlling every fund and stock within the account ourselves. That being said, under the right circumstances, I believe a PHR can complement a physicians own record keeping.
Part II. Microsoft's new HealthValult, More thoughts
I had more time to look at Microsoft's HealthVault. As I mentioned in my last post, after creating my own personal account, I was disappointed by the sparseness of what I saw. There was no place for me to enter my past medical history, medication lists or allergies. As a physician and a software developer, I must admit, I was confused by what I saw. It was not entirely obvious from the look and feel as to what the application really does.
I was hoping for a robust PHR. In fact, I was hoping to start signing up my patients for accounts as they presented for their appointments. However, if I found the application confusing, it would be pointless trying enroll my patients at this point.
I looked up all the available information on HealthVault from the Microsoft site. Because of my experience in developing healthcare applications, I believe I have a fair understanding of this application now. However, for many, I believe the application is a bit obtuse. I think it's fair to say, HealthVault, despite a barrage of news in the popular media, is not quite ready for direct patient use.
I do remain excited by this offering despite my early disappointment. Having a large company like Microsoft leading this effort, I believe there will be more opportunities for independent developers to create new healthcare applications. I know many think Microsoft is trying to "take over" healthcare, but I'm trying to take the positive view. We'll just have to wait and see.
More on HealthVault later...
I was hoping for a robust PHR. In fact, I was hoping to start signing up my patients for accounts as they presented for their appointments. However, if I found the application confusing, it would be pointless trying enroll my patients at this point.
I looked up all the available information on HealthVault from the Microsoft site. Because of my experience in developing healthcare applications, I believe I have a fair understanding of this application now. However, for many, I believe the application is a bit obtuse. I think it's fair to say, HealthVault, despite a barrage of news in the popular media, is not quite ready for direct patient use.
I do remain excited by this offering despite my early disappointment. Having a large company like Microsoft leading this effort, I believe there will be more opportunities for independent developers to create new healthcare applications. I know many think Microsoft is trying to "take over" healthcare, but I'm trying to take the positive view. We'll just have to wait and see.
More on HealthVault later...
Thursday, October 4, 2007
Microsoft's new Health Valult, a PHR?
I received notification about this new offering by Microsoft, "Health Vault". Dr Crounse, Worldwide Health Director for the Microsoft, writes about it in his blog.
As a practicing physician, I'm really excited about this application and have signed up for a personal account. My plan is to start enrolling my patients with the hope of consolidating their medical data.
I found however that the application did not have a place for me to enter my past medical history, medication lists etc. I think, for this application to work for my patients, this feature needs to be in place. Perhaps this feature already exists. If this is the case, it needs to be more obvious to the user. I know this is in beta, so I'm willing to wait. My hope is that the Health Vault is a true PHR.
There is an interesting integration feature. I can fax documents to my patient's account using a fax subscription service that converts the faxed document to a PDF file for storage in the patient's Health Vault. The patient must subscribe to the service. The cost is very reasonable however.
I will write more about the HealthVault as I discover more of its features.
As a practicing physician, I'm really excited about this application and have signed up for a personal account. My plan is to start enrolling my patients with the hope of consolidating their medical data.
I found however that the application did not have a place for me to enter my past medical history, medication lists etc. I think, for this application to work for my patients, this feature needs to be in place. Perhaps this feature already exists. If this is the case, it needs to be more obvious to the user. I know this is in beta, so I'm willing to wait. My hope is that the Health Vault is a true PHR.
There is an interesting integration feature. I can fax documents to my patient's account using a fax subscription service that converts the faxed document to a PDF file for storage in the patient's Health Vault. The patient must subscribe to the service. The cost is very reasonable however.
I will write more about the HealthVault as I discover more of its features.
Results Managemenent, Critical results reporting
Clinical test reporting is a big issue for physicians. As a physician based in an ambulatory office, I may have several patients at any given time undergoing various radiology tests such as a chest x-rays or CT scans. When the results are normal, it's okay to receive the results by routine fax or ground mail. Potential problems however occur when there's an abnormal result that needs follow-up.
Although many times these critical results are also faxed to the doctor, this really is not an acceptable way of communicating a result needing follow-up. Faxes are notoriously problematic. You can never be sure that the recipient has received the faxed document. After all, fax machines can run out of paper or ink and there is no way for the sender to know that the recipient has received the document.
There needs to be proper follow-up on abnormal test results. By this I mean the radiologist making the abnormal finding should really be calling the ordering physician to review these abnormal findings and to develop a follow-up plan. When results are very high in critical severity, this process usually occurs. When the results may not rank high in the severity scale but are still abnormal, a one-to-one notification method still needs to be in place. There needs to be a system to verify that the abnormal result was received by the appropriate party. An electronic system would be ideal.
If an abnormal result has not been receieved by the appropriate provider, another attempt must take place to convey the results. If all attempts fail, there needs to be further escalation of the process to ensure that a responsible physician is able to act on the abnormal results.
I came across a possible vendor solution to this problem:
"Critical test reporting, closing the loop"
http://www.vocada.com/veriphy-solution.asp
Although many times these critical results are also faxed to the doctor, this really is not an acceptable way of communicating a result needing follow-up. Faxes are notoriously problematic. You can never be sure that the recipient has received the faxed document. After all, fax machines can run out of paper or ink and there is no way for the sender to know that the recipient has received the document.
There needs to be proper follow-up on abnormal test results. By this I mean the radiologist making the abnormal finding should really be calling the ordering physician to review these abnormal findings and to develop a follow-up plan. When results are very high in critical severity, this process usually occurs. When the results may not rank high in the severity scale but are still abnormal, a one-to-one notification method still needs to be in place. There needs to be a system to verify that the abnormal result was received by the appropriate party. An electronic system would be ideal.
If an abnormal result has not been receieved by the appropriate provider, another attempt must take place to convey the results. If all attempts fail, there needs to be further escalation of the process to ensure that a responsible physician is able to act on the abnormal results.
I came across a possible vendor solution to this problem:
"Critical test reporting, closing the loop"
http://www.vocada.com/veriphy-solution.asp
Wednesday, October 3, 2007
Learning from Past HIE / RHIO Mistakes
I just received an eHealth SmartBrief which contained a great editorial from Health Data Management, "Learning From Mistakes" which discusses how we must learn from mistakes of past HIE and RHIOs. The author highlight several points that I also have been making. This did not surprise me when I read that the author, too, like my self, is a practicing physician dealing with the day-to-day chores of clinical data management,
Here a few quotes from the article:
"pioneers in this emerging field concentrated on creating entities, not functionality. " "... they set out to build an organization like a RHIO, rather than advance the attainment of information exchange. "
I have been commenting on this point of how RHIO have been all about setting up large organizations rather then entities that actually do something useful from the physician user perspective.
Another great line from the article:
"With the focus on form, not function, it was easy for participants to get sidetracked with political agendas, competing priorities and administrative processes..."
This reminded me about a recent encounter at a healthcare conference recently, where I met the head of a major EMR vendor's community based initiatives group. While discussing our RHIO initiative, SEMRHIO, I was asked by this vendor representative,"What is your governance model". I smiled and told her, " Our model is about creating real value for the physician , not about by building an organizational structure".
I believe in the "If you build it, they will come" model. Like any great invention, its the idea that comes first, then the organization. After all, Thomas Edison's light bulb came before General Electric.
With RHIOs, we need to focus on "what do our physicians need to enable them to care for their patients?". This should be the guiding principle. It usually takes several iterations to get the right model. Too many development initiatives get locked into a model from the start. RHIOs need to be agile, and have the ability to change or modify the model if required. By having something people really want, the rest should come easy.
Here a few quotes from the article:
"pioneers in this emerging field concentrated on creating entities, not functionality. " "... they set out to build an organization like a RHIO, rather than advance the attainment of information exchange. "
I have been commenting on this point of how RHIO have been all about setting up large organizations rather then entities that actually do something useful from the physician user perspective.
Another great line from the article:
"With the focus on form, not function, it was easy for participants to get sidetracked with political agendas, competing priorities and administrative processes..."
This reminded me about a recent encounter at a healthcare conference recently, where I met the head of a major EMR vendor's community based initiatives group. While discussing our RHIO initiative, SEMRHIO, I was asked by this vendor representative,"What is your governance model". I smiled and told her, " Our model is about creating real value for the physician , not about by building an organizational structure".
I believe in the "If you build it, they will come" model. Like any great invention, its the idea that comes first, then the organization. After all, Thomas Edison's light bulb came before General Electric.
With RHIOs, we need to focus on "what do our physicians need to enable them to care for their patients?". This should be the guiding principle. It usually takes several iterations to get the right model. Too many development initiatives get locked into a model from the start. RHIOs need to be agile, and have the ability to change or modify the model if required. By having something people really want, the rest should come easy.
Tuesday, October 2, 2007
Physician Mobile Device Applications
Anne Zieger, editor of FierceHealthIT, writes in her recent editorial, "Physician mobile device use: It's your move", about the need to develop a suite of mobile applications that serves the needs of physician physicians. Because physicians are always on the go, the mobile device, I believe is ideally suited to a physician's workflow needs.
The problem however is the fact the physicians also need to access a vast array of detailed data when taking care of patients. The challenge with these applications has been with making the data easily accessible on a small mobile device and to do it in an efficient manner so as not to be awkward to use.
There are several very useful applications currently available for the mobile device. The Epocrates (http://www.epocrates.com/) drug data base is probably the most popular application designed for the mobile platform. As a physician, I always have it on me and constantly use it all day long.
Another application, that I feel will be very successful, is the mobile platform for medical education/CME/Case consults by QuantiaMD . What I like about this application, is that as a busy physician on the go, I can listen and watch interesting medical content by Quantia on my Motorola Q-phone. This content can be tailored by Quantia to come from my affiliated hospitals, such as hospital grand rounds. Physicians from my healthcare community can post interesting cases and do short powerpoint presentations which I can access on my mobile device or via the web.
I'd be interested in hearing about other mobile applications.
The problem however is the fact the physicians also need to access a vast array of detailed data when taking care of patients. The challenge with these applications has been with making the data easily accessible on a small mobile device and to do it in an efficient manner so as not to be awkward to use.
There are several very useful applications currently available for the mobile device. The Epocrates (http://www.epocrates.com/) drug data base is probably the most popular application designed for the mobile platform. As a physician, I always have it on me and constantly use it all day long.
Another application, that I feel will be very successful, is the mobile platform for medical education/CME/Case consults by QuantiaMD . What I like about this application, is that as a busy physician on the go, I can listen and watch interesting medical content by Quantia on my Motorola Q-phone. This content can be tailored by Quantia to come from my affiliated hospitals, such as hospital grand rounds. Physicians from my healthcare community can post interesting cases and do short powerpoint presentations which I can access on my mobile device or via the web.
I'd be interested in hearing about other mobile applications.
Subscribe to:
Posts (Atom)




