I've been meaning to comment on this recent item, "Why RHIOs shouldn't exist" from FierceHealthIT. The editor, Anne Zieger, makes a case for her assertion that RHIOs should not exist because they have unrealistic expectations for trust among competing institutions such as hospitals. She states,
"I certainly like the idea of data following me. I love the idea of my providers cooperating. But at the moment, I simply can't see how this kind of data sharing can work in the near future."
Well, patient data sharing is not some novel concept that needs debating. Its already happening, although some do not even realize it. It happens by the fax machine. Patient data sharing is an essential function of caring for patients.
Replacing the fax machine, an inherently in-secure method of data exchange, by a secure electronic exchange is what a RHIOs should be all about The discussion should not be about whether RHIOs should exist, but rather, what is the best model for a RHIO in order to win trust among entities to enable clinical data sharing to take place.
We made a case recently at the recent MSHUG fall Forum 2007, for a RHIO Trust model, which has been very successful in gaining trust among our participants in SEMRHIO.
Friday, September 28, 2007
Thursday, September 27, 2007
Medical Home, a case of the “Emperor’s New Clothes” ?
I’m still trying to understand the concept of the “Medical Home”. To me, all the talk, and there’s plenty, just read the current issue of AMA news, “New Orleans grows into testing ground for medical homes”, it all seems like talk about the “Emperor’s New Clothes”.
So far, what I heard, the medical home concept sounds awfully similar to the concept of the “HMO Health Center” of the 1990’s with the addition of EMRs.
“…continuous care, coordinated care across the health system, utilization of information technology and enhanced care through systems such as open scheduling.”
“…the concept of partnerships between primary care physicians and patients to coordinate access to all needed medical services and consultations (a 'medical home') for all patients."
In the “HMO Health Center” model, the PCP was the “gate-keeper” or care-coordinator. From my experience in managing an “HMO Health Center” during its final days in 1999, we had our own case managers and social workers who helped coordinate the care of our patients. We followed the care of our patient’s from the ambulatory setting, to the hospital, and then to the return to home. We worked closely with our “contracted VNA” (Visiting Nurse Association), hospital case managers, and nursing homes. We had our panel of preferred specialists who helped care for our patients.
What we did not have however, was an electronic medical record or a community health information exchange. I remember being frustrated with not always having right clinical data when I needed it. As a former engineer, I knew then that clinical data access was the one thing that was truly lacking and prevented us from achieving the promise of the HMO health center model of safe, efficient and patient friendly healthcare.
Well, with EMR and health information exchange technology (or RHIO), I hope the "Medical Home" does not turn out to be a case of the "Emperor’s new Clothes".
If you are trying to understand the Medical Home concept, check these :
Medical Home Concept Catching on in the US a Washington Post Article
Medical Home Concept Paper An in depth paper from the state of Louisiana
Waye and Means, Medical Home
eCareManagement Blog item on Medical Home
The Patient-Centered Primary Care Collaborative : coalition of major employers, consumer groups, and other stakeholders who have joined with organizations representing primary care physicians to develop and advance the patient centered medical home.
So far, what I heard, the medical home concept sounds awfully similar to the concept of the “HMO Health Center” of the 1990’s with the addition of EMRs.
“…continuous care, coordinated care across the health system, utilization of information technology and enhanced care through systems such as open scheduling.”
“…the concept of partnerships between primary care physicians and patients to coordinate access to all needed medical services and consultations (a 'medical home') for all patients."
In the “HMO Health Center” model, the PCP was the “gate-keeper” or care-coordinator. From my experience in managing an “HMO Health Center” during its final days in 1999, we had our own case managers and social workers who helped coordinate the care of our patients. We followed the care of our patient’s from the ambulatory setting, to the hospital, and then to the return to home. We worked closely with our “contracted VNA” (Visiting Nurse Association), hospital case managers, and nursing homes. We had our panel of preferred specialists who helped care for our patients.
What we did not have however, was an electronic medical record or a community health information exchange. I remember being frustrated with not always having right clinical data when I needed it. As a former engineer, I knew then that clinical data access was the one thing that was truly lacking and prevented us from achieving the promise of the HMO health center model of safe, efficient and patient friendly healthcare.
Well, with EMR and health information exchange technology (or RHIO), I hope the "Medical Home" does not turn out to be a case of the "Emperor’s new Clothes".
If you are trying to understand the Medical Home concept, check these :
Medical Home Concept Catching on in the US a Washington Post Article
Medical Home Concept Paper An in depth paper from the state of Louisiana
Waye and Means, Medical Home
eCareManagement Blog item on Medical Home
The Patient-Centered Primary Care Collaborative : coalition of major employers, consumer groups, and other stakeholders who have joined with organizations representing primary care physicians to develop and advance the patient centered medical home.
Wednesday, September 26, 2007
Performance Reporting on Lab data
A challenge for many provider and managed care organizations is reporting on lab data for P4P and quality initiatives. Lab data usually is available as HL7 2.x formatted data. Just the term "HL7" can be scary. Extracting (or parsing out) lab data from HL7 usually involves the use of expensive and complex tools, such as an HL7 interface engine. Aside from the cost, there is a steep learning curve for understanding and working with HL7.
If batch reporting is your main need, the CALINX Lab import tool may be for you. It converts HL7 v2.x lab data to a "flat-file". A flat file is essentially just a comma-delimited data file. Most "MS-Access" programmers are familiar with importing this type of data file into a database. Its certainly easier to work with lab data in this format. Check out the Calinx guide, which provides a very straight forward description of the Calinx lab data standard and provides an excellent primer on HL7 v2x lab data.
If batch reporting is your main need, the CALINX Lab import tool may be for you. It converts HL7 v2.x lab data to a "flat-file". A flat file is essentially just a comma-delimited data file. Most "MS-Access" programmers are familiar with importing this type of data file into a database. Its certainly easier to work with lab data in this format. Check out the Calinx guide, which provides a very straight forward description of the Calinx lab data standard and provides an excellent primer on HL7 v2x lab data.
RHIOs are still relevant according to Dr Brailer
Neil Versel, who is also a fellow health IT blogger listed on HITSphere, just wrote an article, for Digital HealthCare & Productivity: "Brailer Insists RHIOs Remain Important".
Dr Brailer still remains bullish on the prospects of RHIOs. He admits that RHIOs are undergoing a shakedown. I also believe this is the case.
Take the dot-com boom as an example. The initial exuberance was followed by people questioning whether the Internet could actually produce a sustainable business model. Well, since then we have seen the likes of Amazon.com, Google.com, youTube.com, and the list keeps growing.
RHIOs too, I believe will follow a similar path. Just as with the dot-coms, when funding was abundant, there was a "spend-spend" mentality without regards to sustainability. RHIOs, like the dot-coms, had been flush with significant funding, mainly from state and federal grants. In fact, there is a term for these grant-dependent entities: "Beltway bandits – a group of people who live off government grants", "grant babies" (see HISTalk)
The Santa Barbara RHIO is a good example, where it did not take long to burn through $10M in funding, only to learn in the end, that there really did not seem to be a need for such an entity in their community. Just recently, we learned of the shutting down of the Oregon RHIO, which did so only after spending nearly $500K just to find out that their RHIO was going to be to expensive.
Once you start hiring those consultants and lawyers, and start setting up committees, money can dry up very fast. RHIOs need to evolve, I believe from an entrepreneurial model that enabled the small technology start-ups in the 80s and 90's to beat the larger companies. After all, it was this model that allowed IBM to develop the now famous IBM Personal Computer (IBM-PC). IBM, in the early 80s, after learning from the success of Apple Computer, used a "small start-up company" model to develop the IBM-PC.
RHIOs will start to succeed once they focus on sustainable models that meet true business needs rather than needs decided by committees. They will need to adopt a "start-up" model, depend less on government funding (handouts), and rely more on self-funding and private investments.
Dr Brailer still remains bullish on the prospects of RHIOs. He admits that RHIOs are undergoing a shakedown. I also believe this is the case.
Take the dot-com boom as an example. The initial exuberance was followed by people questioning whether the Internet could actually produce a sustainable business model. Well, since then we have seen the likes of Amazon.com, Google.com, youTube.com, and the list keeps growing.
RHIOs too, I believe will follow a similar path. Just as with the dot-coms, when funding was abundant, there was a "spend-spend" mentality without regards to sustainability. RHIOs, like the dot-coms, had been flush with significant funding, mainly from state and federal grants. In fact, there is a term for these grant-dependent entities: "Beltway bandits – a group of people who live off government grants", "grant babies" (see HISTalk)
The Santa Barbara RHIO is a good example, where it did not take long to burn through $10M in funding, only to learn in the end, that there really did not seem to be a need for such an entity in their community. Just recently, we learned of the shutting down of the Oregon RHIO, which did so only after spending nearly $500K just to find out that their RHIO was going to be to expensive.
Once you start hiring those consultants and lawyers, and start setting up committees, money can dry up very fast. RHIOs need to evolve, I believe from an entrepreneurial model that enabled the small technology start-ups in the 80s and 90's to beat the larger companies. After all, it was this model that allowed IBM to develop the now famous IBM Personal Computer (IBM-PC). IBM, in the early 80s, after learning from the success of Apple Computer, used a "small start-up company" model to develop the IBM-PC.
RHIOs will start to succeed once they focus on sustainable models that meet true business needs rather than needs decided by committees. They will need to adopt a "start-up" model, depend less on government funding (handouts), and rely more on self-funding and private investments.
Tuesday, September 25, 2007
More new on ICU Telemedicine
I just read an article on ICU telemedicine in the recent issue of AMA news,
AMA News: Big hospitals adding remote monitoring for ICU patients
The article describes the e-ICU implementation at the University of Massachusetts Memorial Medical Center. VISCU, an ICU telemedicine systems company that I described in an earlier post, is the apparently the only vendor selling such systems. The article states that more than 200 hospitals use it to monitor 250,000 patients a year.
Some of the drivers for ICU telemedicine is the growing physician shortage and new patient safety initiates. I can certainly can testify to the fact that with the increased emphasis on patient safety, and the new medicare policy for "no payment for medical errors", we will see the growth of telemedince and other advanced monitoring technologies.
Some of the benefits seen from introducing ICU telemedicine at the UMASS Memorial Medical center were:
1- decline of pneumonia rates
2- decrease in deaths by 9%
3-decrease in length of stay
4- decrease in ventilator-associated pneumonia to 1/4th the national average.
These results are impressive. If they also translate to cost savings or increased patient volume, more hospitals and other healthcare facilities will be incentivized to further adopt telemedicine services.
AMA News: Big hospitals adding remote monitoring for ICU patients
The article describes the e-ICU implementation at the University of Massachusetts Memorial Medical Center. VISCU, an ICU telemedicine systems company that I described in an earlier post, is the apparently the only vendor selling such systems. The article states that more than 200 hospitals use it to monitor 250,000 patients a year.
Some of the drivers for ICU telemedicine is the growing physician shortage and new patient safety initiates. I can certainly can testify to the fact that with the increased emphasis on patient safety, and the new medicare policy for "no payment for medical errors", we will see the growth of telemedince and other advanced monitoring technologies.
Some of the benefits seen from introducing ICU telemedicine at the UMASS Memorial Medical center were:
1- decline of pneumonia rates
2- decrease in deaths by 9%
3-decrease in length of stay
4- decrease in ventilator-associated pneumonia to 1/4th the national average.
These results are impressive. If they also translate to cost savings or increased patient volume, more hospitals and other healthcare facilities will be incentivized to further adopt telemedicine services.
Friday, September 21, 2007
Discussing Healthcare data exchange on Deb Zona's "Healthcare in Crisis" show
I was recently on Deb Zona's Cable TV show, "Health Care in Crisis" with my partner, Dr Louis Maggio, where we discussed problems and issues regarding the management of clinical data and healthcare data exchange.
The purpose of our discussion was to describe in very simple terms, the problem that is faced by physicians, patients and care-givers in trying to keep track of a patient's clinical data including medication lists. We used this discussion to serve as a laymans introduction to the concept of a RHIO or HIE.
Clip1
Dr Maggio discusses Medication Reconciliation and how patients manage their own medication lists.
Clip 2
Some points discussed:
Clip 1:
The purpose of our discussion was to describe in very simple terms, the problem that is faced by physicians, patients and care-givers in trying to keep track of a patient's clinical data including medication lists. We used this discussion to serve as a laymans introduction to the concept of a RHIO or HIE.
Clip1
Dr Maggio discusses Medication Reconciliation and how patients manage their own medication lists.
Clip 2
Some points discussed:
Clip 1:
- Patient clinical data is spread out throughout the community, at the various hospitals, imaging centers, labs etc.
- Patients in their healthcare, can undergo multiple care transitions during their illness. These transitions may include home to hospital, to nursing home/rehab, to home with VNA and finally back home under previous arrangemnt.
- Challenge for the physician and the patient/care-givers, is keeping track of the data that is generated at each of these care settings. It is critical not to lose track of any data as care settings change.
- It is importany to maintain a unified view of the patient regardless of the care setting.
Wednesday, September 19, 2007
Home telemonitoring, new study released
See Telemedicine works which was forwarded to me by FierceHealthIT.
Here is what was said:
Here is what was said:
"Home telemonitoring of chronic diseases appears to
be a promising approach to patient management, says a team of Canadian scholars
who reviewed more than 65 telemonitoring studies in the United States and
Europe..."
"The 65 papers they examined included studies on
the home-based management of chronic pulmonary conditions, cardiac diseases,
diabetes, and hypertension. Each of the studies employed various information
technologies that were used to monitor patients at a distance.
"
"The study, entitled “Systematic Review of Home
Telemonitoring for Chronic Diseases: The Evidence Base,” appeared in the
May/June 2007 issue of the Journal of the American Medical Informatics
Association. "We need more studies like this to generate interest in this area and to really help telemedicine become a "standard of care".
Telemedicine in Diabetic Disease Management
Just read an article forwarded to me by FierceHealth, "Trend: Managing chronic diseases remotely, with mobile tech". Devices will play a big role in remote patient monitoring and disease management. Diabetes is a perfect example. An electronic device, the Glucometer plays a central role in the management of diabetes, unlike, say Rheumatoid arthritis, a condition for which there is no electronic device for monitoring. What a great way to combine diabetic management with existing communication technologies by building a glucometer into a cellphone and taking advantage of the remote monitoring capabilities.
See this article: "Trend: Managing chronic diseases remotely, with mobile tech":
See this article: "Trend: Managing chronic diseases remotely, with mobile tech":
"HealthPia's GlucoPhone, which combines a glucometer with a cell phone, is being used by fewer than 100 patients nationwide since FDA granted it premarket approval last year. HealthPia charges $79 as part of an introductory package for its GlucoPhone, as long as patients also pay for the service from its selected
telephone carrier, LogicMobile. Patients also have to purchase testing strips
that must be used in conjunction with the phone, although Medicare reimburses
patients for the strips."
Telemedicine in the ICU

I just came across some good links on Telemedicine ICU applications:
Check out the Doctors who developed the use of an ICU Telemedicine system used at Penn developed by a company, Visicu, the "eICU system" (Visicu, like "Visual ICU") .
Take a look at their technical architecture diagram.
Notice the similaries with RHIO technical architectural diagrams. Same HL7 challenges etc. Again, I see Telemedicine as a natural extension of disparate clinical data integration challenge.
In an earlier post, I mentioned how, because of lack of payer reimbursement for telemedicine, the costs may be borne out by facilities such as hospitals because of a perceived notion that telemedicine brings better outcomes and as a result reduced costs. This is apparently the case at Penn's Telemedicine ICU:
Doc in a Box blog writes:
"And also we must not forget about whether we can
bill for this service. Presently the hospital supports it based on the notion
that increased quality saves money."
The Telemedicine Market
Just came across this article on Telemedicine market prospects while reading the Telemedicine, Telehealth, and the TIE blog:
Broadband where it’s never gone before and other technological marvels
by Jonathan Blum, April 2007 issue
The real challenge that I have found is exactly the physician-business part. The "doctor's business" is very different from any other business. It is not strictly a consumer-driven, price sensitive business. We have third party payers, the insurance companies, which tend to drive healthcare spending depending on what services they cover and the reimbursement amount. I do not expect patients to pay for these telemedicine services themselves. More likely, it will be the payers or healthcare facilities, such as hospitals and nursing homes that would pay for these services if they see some improved outcome or cost saving.
The promise of telemedicine is delivering timely healthcare that meets the demand of the patient's illness. Similar to the concept of the "on demand service" concept that we see in the general IT space. With more timely medical interventions, patients would experience fewer treatment delays, less complications and thus reduced overall costs. If we can make this case, I'm sure we'll see the payers move faster in this direction.
Broadband where it’s never gone before and other technological marvels
by Jonathan Blum, April 2007 issue
"The Ultimate UCG: Telemedicine
Think user-created video
and music are hot? Meet telemedicine.
Sometimes called digital medicine
or remote monitoring, the process of providing health care remotely via the Web
is a massive market that is finally beginning to organize.
Around 60 million
people in the United States suffer from a chronic illness, according to
Dallas-based research firm Parks Associates. Factor in those providing care and
the total audience for health care can easily double, or even triple, that
figure.
With the potential audience that high, the telemedicine market is
expected to grow to $1.83 billion by 2010, according to Parks Associates’
research analyst Harry Wang. And companies like adt’s QuietCare and Webvmc are offering services such as remote
monitoring, in-home wellness, and the Remote Nurse — a purpose-built health-care
display.
“The technology behind the industry has been in place for 15
years,” says Wang. “What holds it back is the lack of
understanding of the business between doctors, insurers and patients.”
In other words, a few good branding campaigns
could help this nascent industry grow into a real market. "
The real challenge that I have found is exactly the physician-business part. The "doctor's business" is very different from any other business. It is not strictly a consumer-driven, price sensitive business. We have third party payers, the insurance companies, which tend to drive healthcare spending depending on what services they cover and the reimbursement amount. I do not expect patients to pay for these telemedicine services themselves. More likely, it will be the payers or healthcare facilities, such as hospitals and nursing homes that would pay for these services if they see some improved outcome or cost saving.
The promise of telemedicine is delivering timely healthcare that meets the demand of the patient's illness. Similar to the concept of the "on demand service" concept that we see in the general IT space. With more timely medical interventions, patients would experience fewer treatment delays, less complications and thus reduced overall costs. If we can make this case, I'm sure we'll see the payers move faster in this direction.
Saturday, September 15, 2007
IT Workers with Server Virtualization Skills in High Demand
I recently blogged about server virtualization on my Virtualization for "dummies" post. Well the HIS-Talk blog took me to this article: Help wanted: IT workers with server virtualization skills
Now I knew Virtualization was somehow going to tie back to healthcare, and RHIOs, even though it seems strictly a "techie" topic. Here is mention of HealthBridge, one of the few self sustaining RHIOs in the country:
Virtualization for RHIOs
Benefits of Virtualization:
Now I knew Virtualization was somehow going to tie back to healthcare, and RHIOs, even though it seems strictly a "techie" topic. Here is mention of HealthBridge, one of the few self sustaining RHIOs in the country:
Virtualization for RHIOs
Demand for IT workers"Jeff Perry, IT manager at HealthBridge, a
not-for-profit organization in Cincinnati that electronically connects area
hospitals and other medical facilities so doctors can exchange patient data,
began deploying virtualization software six months ago."
"As more organizations adopt server virtualization
software, they're also looking to hire people who have worked with the
technology in live applications..."
Benefits of Virtualization:
"...after seeing how virtualization has led to
server consolidation, the removal of old hardware and lower power and cooling
costs at Carter & Burgess, Youngers is convinced that it's a need-to-know
technology for IT workers. "You are going to have to get on board," he
said."If you're interested in Virtualization in Healthcare, read on: Here is an opinion paper by IBM on Virtualization in Healthcare.
XDS HE Architecture: Central vs Distributed Repository
Setting up an XDS Affinity Domain using IHE Components: This IBM Healthcare and Life Sciences document has some nice practical information on IHE XDS.
Here are two diagrams taken from this document showing a Centralized vs a Distributed repository architecture.
Centralized Repository: Note that the "Document Repository" object is contained within the "Infrastructure Provider" along side the "Document Registry".
 Figure 1
Figure 1
Distributed Repository : Here the "Document Repository" is now contained within each hospital's infrastructure while the "Document Registry" still remains within the centrally located "Infrastructure Provider".
 Figure 2
Figure 2
Here are two diagrams taken from this document showing a Centralized vs a Distributed repository architecture.
Centralized Repository: Note that the "Document Repository" object is contained within the "Infrastructure Provider" along side the "Document Registry".
 Figure 1
Figure 1Distributed Repository : Here the "Document Repository" is now contained within each hospital's infrastructure while the "Document Registry" still remains within the centrally located "Infrastructure Provider".
 Figure 2
Figure 2So what does this all mean ? By "Central Repository", I mean a central, single database that contains all the documents in the enterprise. The "Distributed Repository" implies multiple databases. These databases can be centrally located however , within a single data center. This would still be a "Distributed Repository" since each repository sits in its own database.
What is the advantage of this model ? You can best understand this by comparing it to "Google". When we perform a search in Google, the search term goes out to an index of terms within Google's infrastructure. This "index" in analogous to the "Document Registry". The index or registry contains links (or addresses) to the locations of the actual data. The actual data may reside at different servers throughout the world. This "Distributed Repository" model works the same way, and just like Google, it can scale infinitely.
Because of the scalability of this "Distributed Model", this model can be the basis of a "SaaS architecture" where there is a need to be able to scale to meet the needs of a rapidly growing user base.
Once again, please check out this IBM document for more information.
Also, here are some other useful IBM documents: Clinical Imaging Repositories, Solution Architecture for Clinical Data Management
Cross Enterprise Document Sharing: IHE XDS Integration
Microsoft IHE XDS Reference Implementation
 I will be sharing information on Cross enterprise document sharing which is an important topic in the area of Health Information Exchanges and RHIOs. This model would equally apply to single organiziation document sharing as well.
I will be sharing information on Cross enterprise document sharing which is an important topic in the area of Health Information Exchanges and RHIOs. This model would equally apply to single organiziation document sharing as well.
Microsoft has recently released the IHE, XDS Reference implementation .
Roberto Ruggeri (a Senior Technical Strategist with Microsoft Worldwide Health) has an excellent introduction to IHE XDS on his blog.
Roborto writes:
"Integrating the Healthcare
Enterprise (IHE) is an organization
operating in the Health Information and Communication Technology area. The main
purpose of IHE is to create Interoperability Profiles that simplify integration
scenarios in healthcare."
"Arguably one of the most successful IHE profiles
is Cross-Enterprise Document Sharing or XDS. The profile focuses of the
publication, storage and retrieval of documents for the purpose of exchange
within a network of trusted participants (Affinity
Domain)."
IHE IT Infrastructure Technical Framework
Microsoft IHE, XDS Reference implementation
I found the presentations listed below useful for understanding IHE XDS basics concepts. It would be useful to review these documents before diving into Microsoft IHE, XDS Reference implementation .
IHE Canada, XDS Integration Profile, Technical Discussion
IHE XDS, Presentation by Jonathon L. Ellion MD (Heartlab): Very good , dynamic powerpoint introduction to IHE XDS
Leveraging IHE to Build RHIO Interoperability, Charles Parisot's (GE Healthcare) presentation discusses IHE issues as they relate to RHIOs
This article discusses a strategy for extending the IHE XDS for support of a federated architecture.
Enhancing IHE XDS for Federated Clinical Affinity Domain Support
Setting up an XDS Affinity Domain using IHE Components: This is an IBM Healthcare and Life Sciences document. It's a good practical guide to setting up a theoretical deployment. It addresses the architectural issues involved. Some of the points discussed are:
1. Patient Identity Cross Reference Manager
HIE/RHIO Resources:
MA-SHARE Record Locator Service Technical Document
RHIO Reference Architecture Very good technical discussion of a RHIO architecture. Includes discussions on the use of BizTalk and data flow in a federated architecture model.
 I will be sharing information on Cross enterprise document sharing which is an important topic in the area of Health Information Exchanges and RHIOs. This model would equally apply to single organiziation document sharing as well.
I will be sharing information on Cross enterprise document sharing which is an important topic in the area of Health Information Exchanges and RHIOs. This model would equally apply to single organiziation document sharing as well.Microsoft has recently released the IHE, XDS Reference implementation .
Roberto Ruggeri (a Senior Technical Strategist with Microsoft Worldwide Health) has an excellent introduction to IHE XDS on his blog.
Roborto writes:
"Integrating the Healthcare
Enterprise (IHE) is an organization
operating in the Health Information and Communication Technology area. The main
purpose of IHE is to create Interoperability Profiles that simplify integration
scenarios in healthcare."
"Arguably one of the most successful IHE profiles
is Cross-Enterprise Document Sharing or XDS. The profile focuses of the
publication, storage and retrieval of documents for the purpose of exchange
within a network of trusted participants (Affinity
Domain)."
IHE IT Infrastructure Technical Framework
Microsoft IHE, XDS Reference implementation
I found the presentations listed below useful for understanding IHE XDS basics concepts. It would be useful to review these documents before diving into Microsoft IHE, XDS Reference implementation .
IHE Canada, XDS Integration Profile, Technical Discussion
IHE XDS, Presentation by Jonathon L. Ellion MD (Heartlab): Very good , dynamic powerpoint introduction to IHE XDS
Leveraging IHE to Build RHIO Interoperability, Charles Parisot's (GE Healthcare) presentation discusses IHE issues as they relate to RHIOs
This article discusses a strategy for extending the IHE XDS for support of a federated architecture.
Enhancing IHE XDS for Federated Clinical Affinity Domain Support
Setting up an XDS Affinity Domain using IHE Components: This is an IBM Healthcare and Life Sciences document. It's a good practical guide to setting up a theoretical deployment. It addresses the architectural issues involved. Some of the points discussed are:
1. Patient Identity Cross Reference Manager
2. Security and Auditing
3. Physical and Logical Topology
4. Document Sharing Scenarios
HIE/RHIO Resources:
MA-SHARE Record Locator Service Technical Document
RHIO Reference Architecture Very good technical discussion of a RHIO architecture. Includes discussions on the use of BizTalk and data flow in a federated architecture model.
Friday, September 14, 2007
Telemedicine Service Providers: Partners Telemedicine
Partners Telemedicine, a division of Partners Healthcare, is the leading Telemedicine provider in the country. You can find the cost of their consultation services here.
They have an organization, the "Center for Connected Health" which hosts a number of events including an annual symposium. This year, Symposium 2007 is being held on October 22-23, 2007. The fee is $595 for the 2 day event. The agenda includes discussions on chronic care, international progress, funding, remote patient monitoring etc.
They have an organization, the "Center for Connected Health" which hosts a number of events including an annual symposium. This year, Symposium 2007 is being held on October 22-23, 2007. The fee is $595 for the 2 day event. The agenda includes discussions on chronic care, international progress, funding, remote patient monitoring etc.
Telemedicine Service Providers
I will be listing companies that provide telemedicine services. I just came across Secure Telemedicine
They appear to be appealing to consumers (patients).
This company connects patients with doctors via telemedicine. The company is marketing to patients by offering them a convenient way to consult with a doctor remotely:
"We use technology to bridge the distance between doctors and
patients in need. We look forward to helping you and your family take better care of your health"
How do they Partner with Doctors?: They allow doctors and PAs (Physicians Assistants) to supplement their incomes by providing consultations on a full or part-time basis to Secure Telemedicine's patients. They call it the "Telemedicine Consultation Program (TCP)".
Reasons why a doctor would want to Partner: They make a pitch to doctors who are semi-retired/retired, want to work from home, want to expand their current practice.
My question regarding this model, being a physician in practice, is how much work can I realistically expect ? If I were to just get 1 or 2 consults per day, would the extra effort required to perform this service be worth the small potential payback? My experience with patients is that they generally do not want to spend extra money for these type of extra medical services. They can usually speak to their own physicians regarding their medical issues. I know patients always complain about not being able to access their physicians, but when it comes to paying the extra $30 to $60 (or what ever the payment is) I'm not sure how many takers there really are.
Here's how Secure Telemedicine describe their telemedicine process on their website:
They appear to be appealing to consumers (patients).
This company connects patients with doctors via telemedicine. The company is marketing to patients by offering them a convenient way to consult with a doctor remotely:
"We use technology to bridge the distance between doctors and
patients in need. We look forward to helping you and your family take better care of your health"
How do they Partner with Doctors?: They allow doctors and PAs (Physicians Assistants) to supplement their incomes by providing consultations on a full or part-time basis to Secure Telemedicine's patients. They call it the "Telemedicine Consultation Program (TCP)".
Reasons why a doctor would want to Partner: They make a pitch to doctors who are semi-retired/retired, want to work from home, want to expand their current practice.
My question regarding this model, being a physician in practice, is how much work can I realistically expect ? If I were to just get 1 or 2 consults per day, would the extra effort required to perform this service be worth the small potential payback? My experience with patients is that they generally do not want to spend extra money for these type of extra medical services. They can usually speak to their own physicians regarding their medical issues. I know patients always complain about not being able to access their physicians, but when it comes to paying the extra $30 to $60 (or what ever the payment is) I'm not sure how many takers there really are.
Here's how Secure Telemedicine describe their telemedicine process on their website:
"By logging into a secure physician administration page, the physician will pull up his Telemedicine Case Queue containing 10-50 new telemedicine cases with medical records, histories and possible refill requests. Each case will have three possible components:
- EMR Review (Physician review)
- Teleconsult (Physician consults patient by phone)
- E-prescribing"
"During the teleconsult, the physician will consult with the patient and discuss case, condition and history, and decide on a proper course of action. The Consulting Physician's job is to evaluate the medical history and condition information in each case, and based on that review either:
- Approve
- Reject
- Put on hold and request be faxed an update of the patient medical history if one is necessary; call the patient and verify any additional information deemed necessary; or order a medical exam to continue the medical evaluation."
"If a patient requests prescription medication, the telemedicine physician will review all medical records and make a recommendation."
Thursday, September 13, 2007
RHIOs, HIEs and Telemedicine
A HIMSS Presentation on RHIOs and Telehealth/Telemedicine
The presentation makes the following points:
The presentation makes the following points:
Telemedicine & RHIOs
• RHIOs can integrate Telemedicine
programs into the local health information
exchange
• Telemedicine will create efficiencies, improve
quality and give rural patients better ACCESS
• RHIOs can tie patients to specialists around
the country and the world through TelemedicineTelemedicine Benefits to RHIO
• Increased diagnostic resources
• Improved quality of medical services
• Strengthened ties to specialty care
• Alleviated isolation of rural providers
• Enhanced ability to attract and keep primary care
physicians and staff• Facilitated training of health professionals in rural
communities • Patients can stay close to home for their careAs I mentioned in an earlier post, I see a major function of a RHIOs and HIEs as facilitators of clinical data exchange, moving data from a source provider (hospital, clinical lab etc) to a physician or other healthcare provider. Telemedicine adds to the data services provided by the RHIO.
Telemedicine data

This diagram shows how telemedicine data is just another type of data within the complete clinical dataset. This was taken from a recent telemedicine presentation.
Telemedicine EMR

Here is a screenshot of an EMR used in Telemedicine. It was taken from an ATA 2001 conference presentation. Please refer to Healthcare Vision Inc for information on their products.
Here is a recent presentation (5/2007) and has great EMR screeshots: TeleHealth and EMRs
Dermatology Telemedicine Application (contains very good screenshots):
Wednesday, September 12, 2007
Centralization in a RHIO: a safer, less expensive option for community hospitals
Great quote from: RHIO confidential: Experts offer advice for creating a foolproof privacy and security plan for sharing patient information
The premise for our presentation at Microsoft MSHUG this past August on forming SEMRHIO was that the ability to minimize IT resources by using a "SaaS-like" or centrally hosted services is very important when it comes to forming a RHIO with community based hospitals. Unlike large hospitals systems, community hospital resources are already fairly stretched. These hospitals are not in a postion to manage their own RHIO infrastructure. This is especially important given that most community hospitals already have "too much on their plate" with other higher priority items such as CPOE, eMAR, P4P etc. Forming a RHIO is not exactly seen as a high priority item.
Koss said. “If you’re in a small community where most of the providers are
small and don’t have a lot of resources or technical expertise, then a
centralized service that does that on their behalf might be more secure and
private. By contrast, if you’re in downtown Boston and you’re connecting three
major medical institutions that already have a robust privacy and security
infrastructure, that’s not really an issue.”
The premise for our presentation at Microsoft MSHUG this past August on forming SEMRHIO was that the ability to minimize IT resources by using a "SaaS-like" or centrally hosted services is very important when it comes to forming a RHIO with community based hospitals. Unlike large hospitals systems, community hospital resources are already fairly stretched. These hospitals are not in a postion to manage their own RHIO infrastructure. This is especially important given that most community hospitals already have "too much on their plate" with other higher priority items such as CPOE, eMAR, P4P etc. Forming a RHIO is not exactly seen as a high priority item.
Virtualization for "dummies"
Have you heard that one of the hottest IPO lately is VMware ? What does this company do ? "Virtualization". Whats that ? May be a concept that is hard to grasp initially, but it is an area with great potential to simplify and minimize IT infrastructure. As someone involved in building a RHIO, IT infrastructure costs are a hugh issue and can be a barrier in forming RHIOs and HIEs.
Check this Dell blog item (complete with a video presentation) for a good introduction on Virtualization. Basically, from the dell website on virtualization (not meant to be an advertisement for Dell BTW),
Check this Dell blog item (complete with a video presentation) for a good introduction on Virtualization. Basically, from the dell website on virtualization (not meant to be an advertisement for Dell BTW),
"Virtualization allows you to run multiple applications and operating
systems independently on a single server. Administrators can quickly move
workloads from one virtual workspace to another - easily prioritizing business
needs while maximizing server resources"
Monday, September 10, 2007
EMR Video clip: VistA Integrated Health Care IT
This is an interesting clip with some real life EMR screenshots. Good demonstration of how a patient's electronic medical record is integrated with colonoscopy images and videos, EKG images. Also demonstrates CPOE (computerized physician order entry) for radiology order entry.
Telemedicine Wound Care Video Clip
Wound care is a really neat application of telemedicine. Here is a video clip on the use of telemedicine for wound care. Notice the use of Microsoft's new Ribbon style user interface (Office 2007) in the wound care application.
I wonder if they are using an Office 2007 based application (Infopath or Access) or have developed their own application from "ground-up" ?
A Wound Medicine Project document. Good detailed technical discussion on the design of a wound management application. Allows for on screen measurement of wounds using laser pointers.
I wonder if they are using an Office 2007 based application (Infopath or Access) or have developed their own application from "ground-up" ?
A Wound Medicine Project document. Good detailed technical discussion on the design of a wound management application. Allows for on screen measurement of wounds using laser pointers.
Telemedicine Video clips
Here are a few good video clips on Telemedicine:
Clip #1: A real-life story on the use of Telemedicine consultation in an emergency room where the onsite ER physician was instructed on how to perform a surgical procedure on a critically ill pediatric patient who had just minutes.
Clip #2: Real demo of a Patient's experience with a tele-consultation. This patient presented to a clinic with an ear ache. A nurse used an otoscope connected to the telemedicine equipment (cool) and consulted with a remote Ear Nose and Throat doctor who was able to see the image from the patient's ear.
Clip #1: A real-life story on the use of Telemedicine consultation in an emergency room where the onsite ER physician was instructed on how to perform a surgical procedure on a critically ill pediatric patient who had just minutes.
Clip #2: Real demo of a Patient's experience with a tele-consultation. This patient presented to a clinic with an ear ache. A nurse used an otoscope connected to the telemedicine equipment (cool) and consulted with a remote Ear Nose and Throat doctor who was able to see the image from the patient's ear.
Telemedicine Resources

Telemedicine is another area in health IT that interests me. Being a practicing physician with patients in multiple settings such as nursing homes and hospitals, I believe that telemedicine shows great promise and has yet to reach its potential in transforming how we practice healthcare . It's the combination clinical medicine and cutting edge healthcare IT that is really appealing to a techie physician. Telemedicine technology in many ways is about moving data around between patients and physicians, similar to a RHIO or an HIE.
To me, an HIE (Healthcare Information Exchange) is about moving and aggregating actionable clinical data from multiple data sources to a physician (or other healthcare provider) in order to provider patient care. Telemedicine is just another type of data that must be moved from the source (the patient from the remote location) to the physician.
I will be putting together a list of useful Telemedicine resources. please let me know if I should include anything else.
Telemedicine and Delaying Hospitalization: Interesting item on how telemedicine can reduce hospitalization of nursing home patients from a blog on senior care.
Some interesting points from the blog item:
- "...many doctors have skilled nursing facilities third on their to-do lists"
- “37 percent of the hospitalizations of long-term residents at urban nursing homes nationwide were potentially avoidable.”
- "A doctor can teleconference with a patient, see them via a monitor and make a decision as to what the patient needs."
" Many nursing homes have found this reduces the need for unnecessary hospitalizations.."
More links related to Telemedicine and Hospitalizations:
- Treating Acute Infections by Telemedicine in the Home PDF
- New telemedicine program pairs comfort of home with heart care
- Treating Acute Infections at Home with Telemedicine Presentation on real implementation of telemedicine. Has pictures of the equipment used, list of costs for the equipment and benefits of the program: Shows the reduction in hospital days, costs savings, patient satisfaction etc.
- Telemedicine Information Exchange (TIE) website : Great resource with a wealth of information on Telemedicine.
- Boston Globe article on Nursing home deficiencies and cutting unneeded hospitalizations. How Telemedicine is being used to address these challenges.
Telemedicine in Wound Care
Wound care practice, Woundcare Consultants
Wound care in long term setting from Ostomy Wound Management
Telemedicine Wound care using cell phones
WoundMatrix, wound care EMR
Smith & Nephew's has a Device to measure Wound area. See their website for more information.
Laser device to measure wounds.
Telemedicine Liability: Unfortunately, liability and malpractice are issues that must also be considered even in telemedicine. Here are a few resources:
Blog item on Telemedicine Liability: contains a link to potential liability issues in teleradiology.
Telemedicine Risk makes the following points:
- "...while remote medical practice can bring efficiency and cost savings... it can increase liability."
- "Malpractice insurance is merely the first step in risk management for telemedicine, since local laws may be different on each end of the link..."
Regional Telemedicine Issues
A map of Telemedicine and Telehealth State-by-State: A map with links to each state's telemedicine related issues such as existing programs, reimbursement policies etc.
Arizona's Telemedicine Program, equipment description
Telemedicine in Dermatology
Study using TeleDerm. A comparison of TeleDerm with conventional dermatology.
Telemedicine in Nursing Home
Here is a 2006 presentation on the use telemedicine for nursing home care in the state of Maine.
Employing a Wireless Mobile Solution to Bring
Telemedicine to the Nursing Home Bedside
This is proposal to link three rural Michigan nursing homes via telemedicine.
Northeast Telehealth Resource Center , Partners Healthcare Telemedicine, ME and VT state.
There is a set of document links on their resource page. I have provided them here for convenience.
Informed Consent Reimbursement Policy and Procedures Tele-mental health Protocol for Correctional Inmates Protocol for Medical ASL Interpretation for the Deaf--Video Relay Interpreting Tele-Wound Care Protocol for Nursing Home Residents Tele-Pain management Protocol Tele-pharmacy Protocol
Wound care in long term setting from Ostomy Wound Management
Telemedicine Solution Vendors
REACH Remote Stroke Care
The use a 100% web enabled solution using webs cams, telemedicine carts to deliver reote stroke care to hospital emergency rooms.
InteractiveCare Provides a complete solution for telemedicine. Focus is presently on hospitals but the solution can be deployed in multiple clinical settings. They have a good demo here.
ExhibitOne This company does high definition video conferencing for multiple applications including healthcare.
HealthPia America, Medical Device company. Their flagship product is the "All-in-One Diabetes phone, a cell phone with a built-in glucose monitor that essentially functions as a full-time nurse"
Second Opinion Telemedicine Software: A complete solution for telemedicine consultations.
Telemedicine Radiology:
Team Health is a Tele-Radiology group: "TeamHealth Teleradiology (THTR) was founded in 1991, in Durham, North Carolina, by a group of physicians from Duke University. At that time, the centralized interpretative services group offered reading expertise in MRI and CT for rural physicians who lacked access or experience in these modalities. The group provided 24-hour-a-day coverage, including nights and weekends. THTR was the first and the largest teleradiology company of its kind."
Telemedicine Presentations
TeleHealth and EMRs (5/2007) Makes a good case for telemedicine and its integration with EMRs. Also has a great set of EMR screenshots.
A. Hasan Sapci, M.D at the Telemedicine Resource Center at the University of Michigan Health System has included a comprehensive set of interesting telemedicine technical presentations on his online resume.
Telemedicine for developing countries, MIT developed solution
Telemedicine in Disease Management
Telemedicine in Diabetes
Diabetes Telemedicine/EMR product. Describes the benefits of telemedicine in diabetic care.
Comprehensive discussion of Telemedicine in Diabetes, and the endocrinologist's role
IDEATel- Informatics for Diabetes Education and Telemedicine
Home Telemedicine- A Practical Guide Addresses a number of issues: HIPAA, implementation, nurse case management, provider issues
Telemedicine RHIO
RHIOs, Telehealth & Interop (HIMSS Architects of Change 3/2006) Lists several RHIOs with Telehealth components
Telemedicine Technical Resources:
ICU Telemedicine
ICU Medical Service company using Visicu's technology
Article on Inova Health System, North Dakota adoption of Visicu.
The Value of Provider-to-Provider Telehealth Technologies, CITL
TeleHealth Technologies Report
Reducing emergency department transfers- Reducing transfers from correctional facilities to emergency departments and physician offices
- Reducing transfers from nursing home facilities to emergency departments and physician offices
- Replacing in-person consults with virtual consults
- Reducing redundant and unnecessary laboratory tests
Telemedicine Market Article is a little dated, 2004, but does have an excellent market analysis.
Video Conferencing Solutions Vendors
New and Pre-owned equipment , Video Conference Store
Carries Sony Video Conferencing products
LifeSize, High Definition Video solution. This company has their own product which looks pretty slick. They have several excellent video demos of their product in action. Here is a review of their system.
Telemedicine Programs
MTN Missouri Telehealth Network
University of Iowa , Dept of Family Medicine: Samsung SDS of Korea, a development team at the University of Iowa has developed a Nursing Home Telemedicine system, Colonial Manor in Amana, Iowa. See their system diagram.
Karishma Telemedicine: Program based in India, their brochures are here.
Policies and Procedures for providing telemedicine services in Maine
Telemedicine Equipment
Alaska's AFHCAN user manuals
Sunday, September 9, 2007
EMR - Clinical User Interfaces

Medcin from Medicomp has long been a leader in this area with their clinical Medcin terminology. Here is an example of their user input screen. I learned a lot about clinical user interfaces by reading Medicomp's materials. Some EMR vendor web sites include good screenshots of their user interfaces. I have noticed a lot of vendors have utilized a "Medcin-like "clinical observation documenting style.
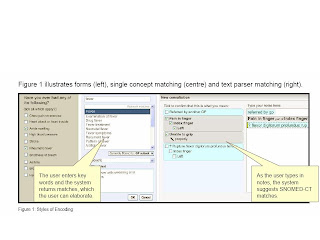
Microsoft has just released a Guidance document for clinical terminology matching for a clinical user interface, which is part of their CUI project: http://www.mscui.net/
They have put together some nice guidance documentation on clinical user controls. I have done a lot of reseach in this area and it is hard to find any comprehensive guidance information regarding clinical user interface development.
Although Medicomp has some good information on their website which includes some nice powerpoint presentations with good screenshots, Microsoft has taken it to the next level. They have made a significant contribution to the clinical IT open-source community by releasing this set of comprehensive clinical user interface guidance documents.

Friday, September 7, 2007
I came across this today:
Mark Hagland is a contributing writer based in Chicago
Sidebar
RHIO Steps to Success—A Sarcastic Look
Are the real RHIO keys to success more about hot air than about healthcare?
The following comes from Mr. HIStalk's blog, http://www.histalk.com/.
Mark Hagland is a contributing writer based in Chicago
Sidebar
RHIO Steps to Success—A Sarcastic Look
Are the real RHIO keys to success more about hot air than about healthcare?
The following comes from Mr. HIStalk's blog, http://www.histalk.com/.
Guide to RHIOs for CIOs, in easy steps:
Participate eagerly in meetings
with your competitors as they talk about sharing data, making sure to speak in
generalities and offering no participation beyond attending more meetings.
Go
back to your co-workers and sneer at how stupid your competitors are and how
backward their systems are compared to yours.
Report back to your fellow VPs
that there's really nothing in it for your organization, but that you'll listen
politely and avoid all commitments just so no one gets mad.
Respond to latest
of 100 surveys asking about RHIOs, making sure to wax poetic about the wonderful
possibilities that will result from the electronic hand-holding that RHIOs will
bring, knowing full well it won't happen until benefits are offered to those
involved.
Go back to your co-workers and make fun of all the folks who've
forgotten CHINs and therefore are doomed to repeat history.
Ignore sales
pitches from vendor RHIO participants who got involved only to troll for new
business.
Go back to your co-workers and make fun of the IT organization of
the local IPA or medical society, consisting of one doctor's brother-in-law
armed with an AA degree and an A-Plus certificate.
Prioritize your IT shop's
involvement in RHIO work somewhere between “get rid of all the cubes and give
everyone an office” and “seriously consider moving all desktops and servers to
open source operating systems.”
Go back to your co-workers and explain to the
bright-eyed among them who ask about RHIOs that it's “no margin, no mission” and
that it will be a cold day in hell when you voluntarily share your exquisitely
created and managed information with the clueless barbarians across town with
their pathetic IT systems.
Get on the speaking circuit and HIMSS advocacy
groups to make sure your attendance at RHIO meetings is rewarded with industry
visibility as a RHIO thought leader.
Subscribe to:
Posts (Atom)




