Another report talking about the cost savings that can be realized by the implementation of telemedicine/telehealth.
Savings of $4.28 billion annually
Fierce Health had some interesting comments on this.
More related items:
California-Could-Become-National-Model-for-Telemedicine
California is the apparent leader in telemedicine. CA will be working on important issues such as reimbursement.
CITL Research
Telehealth Technologies Report Good discussion on the savings and benefits of telemedicine in various care settings: nursing homes, hospitals, correctional facilities etc.
Thursday, November 22, 2007
Wednesday, November 21, 2007
Email Management
We all struggle with email as part of our jobs. I was really amazed to read John Halamka's (CIO Harvard Medical School, BIDH, MASHARE) experience with email. According to his blog, he
receives nearly 600 email a day ! All of which he says are legitimate. John also responds to all of his emails the same day!
Certainly, with the few emails that I have exchanged with John, he always got back to me the same day. He describes in his blog the rules he uses to go through all his emails. I found his method very useful, and have started using some of his techniques in my own email management strategy.
receives nearly 600 email a day ! All of which he says are legitimate. John also responds to all of his emails the same day!
Certainly, with the few emails that I have exchanged with John, he always got back to me the same day. He describes in his blog the rules he uses to go through all his emails. I found his method very useful, and have started using some of his techniques in my own email management strategy.
No Payment for Medical Errors: Massachusetts takes the Pledge
Massachusetts along with Minnesota will no longer be charging patients and payers for "medical errors" as described in this article. This is a new policy announced by Massachusetts Hospital Association (MHA). I had a post on Medicare's no payment policy for medical errors here. The policy is to go in effect October 2008.
The types of medical errors that will not be reimbursed are:
The types of medical errors that will not be reimbursed are:
•Surgery on wrong body part
•Surgery on wrong patient
•Wrong surgical procedure
•Unintended retention of a foreign object
•Patient death or serious disability associated with air embolism that occurs while being treated in a health care facility
•Patient death or serious disability associated with a medication error
•Patient death or serious disability associated with a hemolytic reaction due to administration of incompatible blood or blood products
•Artificial insemination with the wrong donor sperm or wrong egg
•Infant discharged to the wrong family.
This list will be expanded according to the article as more experience is gained in implementing this policy. I did not see much Grey in the list, its fairly black and white. These are all events which are definite errors. Where there may problems, would be in the case of wounds and infections. In these cases, its hard to know if an error actually led to the adverse event. This is the "Grey" area where the implementation of this policy could be problematic.
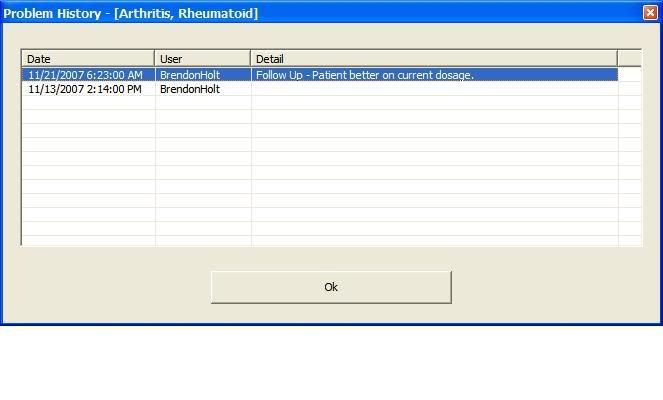
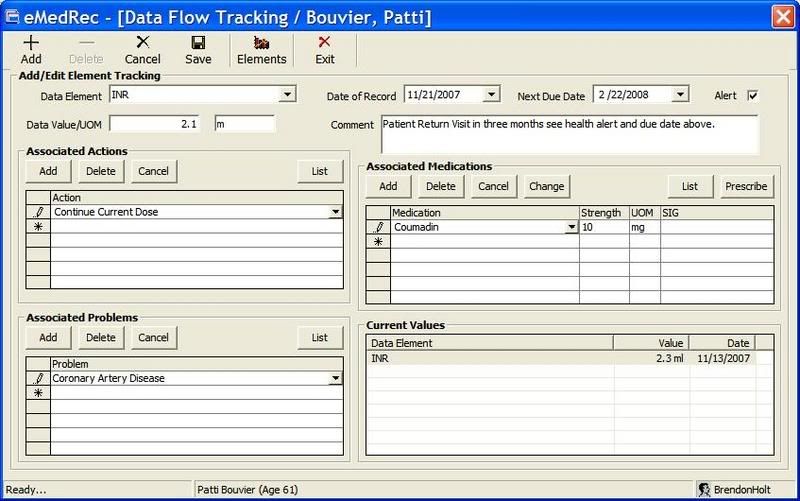
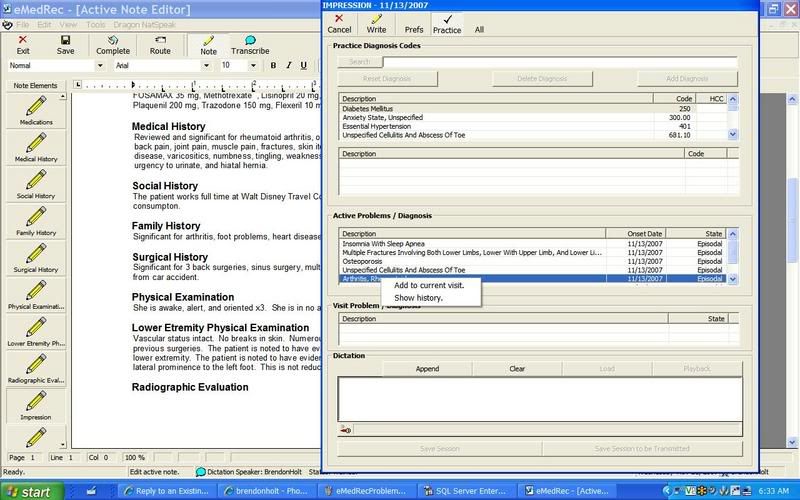
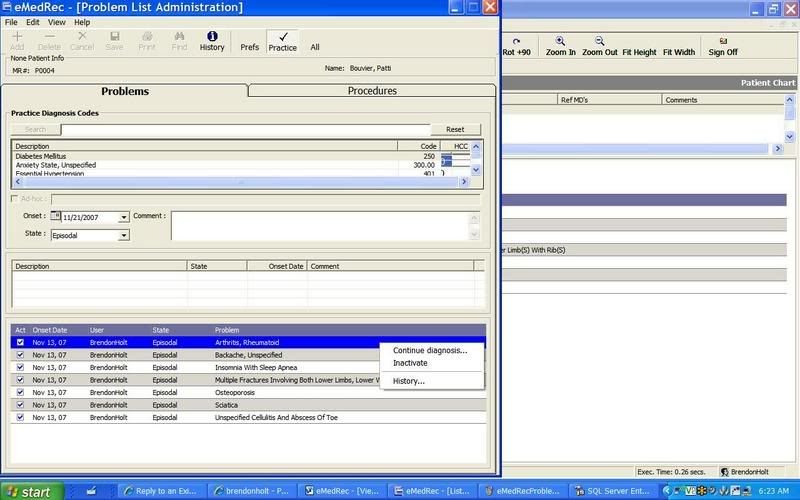
Problem List Management in EMRs



Friday, November 16, 2007
Nursing Home IT
Nursing homes, as suspected, are behind the IT curve according to this article (part 1 of 2). Unfortunately, many nursing homes are barely making it financially. Staffing is always a challenge. Make a transition to electronic systems by nursing homes is too much of a barrier to overcome given these issues.
Wednesday, November 14, 2007
Diabetes Disease Management
Glucometer-in-a-cellphone is a great idea, but I wonder how many people are willing to give up their existing cell phones and all the information that is contained to switch to new phone in order to have it contain a built-in glucometer. I think there needs to be some insurance coverage for this in order for the concept to take off since patients can already get a basic glucometer via their insurance coverage.
Here is a diabetes blog with good information on this topic thats worth looking up.
Here is a diabetes blog with good information on this topic thats worth looking up.
Business Intelligence: Qlikteck in action
Several posts ago I wrote about Qlikteck's Business Intelligence product. Here is an example of Qliktech in action: Fantasy Football.
Sports, especially football and baseball with their wealth of statistics, are a great application of business intelligence.
Sports, especially football and baseball with their wealth of statistics, are a great application of business intelligence.
Monday, November 12, 2007
Document Management Resources
Document Management is a major issue in healthcare. Here is another in the series of "Resource" pages.
ScanGuru, a collection of Document Management information. I found this site to have a wealth of information on document management
Intelligent Routing
Sacnners:
From ScanGuru, Network Scanners: evaluations of 3 network scanners. Price range is $2000-3000. Network scanners allow scan to email, network folder or network fax.
Kodak Scan Station 100: High Volume Network Scanner
- A review of product here.
- Scans direct to search-able PDF, TIFF, folder on network, email or to USB drive.
- Cost approx $2200-2600
- Daily scanning Volume of 1000 pages/day
Document Management Solutions
SpringCM a "SaaS" document management solution
1/14/2010: CVISION, OCR software. Can use for PDF conversion, can watch a folder for changes. Looks like a great product. Can download eval software. I will add more once I test drive it my self.
1/14/2010: Interesting stats on document imaging here. Also see this.
ScanGuru, a collection of Document Management information. I found this site to have a wealth of information on document management
Intelligent Routing
Sacnners:
From ScanGuru, Network Scanners: evaluations of 3 network scanners. Price range is $2000-3000. Network scanners allow scan to email, network folder or network fax.
Kodak Scan Station 100: High Volume Network Scanner
- A review of product here.
- Scans direct to search-able PDF, TIFF, folder on network, email or to USB drive.
- Cost approx $2200-2600
- Daily scanning Volume of 1000 pages/day
Document Management Solutions
SpringCM a "SaaS" document management solution
1/14/2010: CVISION, OCR software. Can use for PDF conversion, can watch a folder for changes. Looks like a great product. Can download eval software. I will add more once I test drive it my self.
1/14/2010: Interesting stats on document imaging here. Also see this.
Thursday, November 8, 2007
RHIO Resources
This will be a page with useful RHIO/HIE resources:
Thanks to Christina for these links:
HIM Principles in Health Information Exchange (Practice Brief)
AHIMA HIM Priciples in Health Information Exchange, Case Scenarios good discussion on MPI, typical use cases. Has some nice diagrams
Continuity of Care (CCR)
Learn more about the Continuity of Care
Update on the CCR Standard TEPR 5/2007
AAFP Center for Health Information IT Has CCR resources
HIMSS Electronic Health Records Vendor Association
"The Continuity of Care Document Quick Start Guide (QSG) is provided free of charge by EHRVA, as a service to vendors and others who will be implementing healthcare documents based on the CCD" : Continuity of Care Document (CCD) Quick Start Guide
Thanks to Christina for these links:
HIM Principles in Health Information Exchange (Practice Brief)
AHIMA HIM Priciples in Health Information Exchange, Case Scenarios good discussion on MPI, typical use cases. Has some nice diagrams
Continuity of Care (CCR)
Learn more about the Continuity of Care
Update on the CCR Standard TEPR 5/2007
AAFP Center for Health Information IT Has CCR resources
HIMSS Electronic Health Records Vendor Association
"The Continuity of Care Document Quick Start Guide (QSG) is provided free of charge by EHRVA, as a service to vendors and others who will be implementing healthcare documents based on the CCD" : Continuity of Care Document (CCD) Quick Start Guide
Visible Body
Just read Chris Paton's blog about Visible Body, coming soon. It says it will be free to use. This looks like it will be a really neat application and I can see myself using it with patients in the exam room.
Wednesday, November 7, 2007
Yahoo, Google and our Privacy, what's there to fear?
This morning I read:
"...Yahoo chief under fire over Chinese dissident ...". Apparently Yahoo provided personal Email data from a Chinese dissident that led to his imprisonment . It really should make you think about just how much of our personal information is out there and what some of the consequences can be when our privacy is compromised.
And just today, I also just read about the Candid CIO's enthusiasm about Google's new StreetView:
"Only a nerd like me would be excited about this"
"It allows you to see 360 pictures of the streets in Google maps. Google has mostly taken pictures of the streets in big cities."
"Yesterday, Just as I was arriving home from work there was a car with a fancy camera mounted on a pole that extended high above the roof. On the side of the car was a magnetic Google sign."
I don't know about you, but I'd get a bit nervous about having Google or any one else having even more info on me. And to think now that we are too also have them keep our personal health records (PHR). We really need to think this through carefully.
"...Yahoo chief under fire over Chinese dissident ...". Apparently Yahoo provided personal Email data from a Chinese dissident that led to his imprisonment . It really should make you think about just how much of our personal information is out there and what some of the consequences can be when our privacy is compromised.
And just today, I also just read about the Candid CIO's enthusiasm about Google's new StreetView:
"Only a nerd like me would be excited about this"
"It allows you to see 360 pictures of the streets in Google maps. Google has mostly taken pictures of the streets in big cities."
"Yesterday, Just as I was arriving home from work there was a car with a fancy camera mounted on a pole that extended high above the roof. On the side of the car was a magnetic Google sign."
I don't know about you, but I'd get a bit nervous about having Google or any one else having even more info on me. And to think now that we are too also have them keep our personal health records (PHR). We really need to think this through carefully.
Tuesday, November 6, 2007
BizTalk, HL7
Eric Stott, a well known BizTalk and HL7, EDI expert who I have the pleasure to work with currently in a health information exchange initiative, has a new website:
hl7-info.com – General HL7 issues, debugging HL7 messages and how BizTalk interacts with the messages
biztalk-info.com – general BizTalk issues, HIPAA related issues
hl7-info.com – General HL7 issues, debugging HL7 messages and how BizTalk interacts with the messages
biztalk-info.com – general BizTalk issues, HIPAA related issues
Monday, November 5, 2007
Physicians Required to Implement an EMR
An interesting item on EMR and HIPAA regarding the decision by Partners Healthcare to require physicians in the network to have an EMR or else leave the network.
I would prefer if they let physicians buy their own EMRs and not have it subsidized. It will be interesting to see how things work out over the next 3-5 years. Technology is changing rapidly. Microsoft and Google are also getting more into healthcare. EMRs available today may appear ancient compared to the new crop of EMRs coming out over the next few years. Buying an EMR today compared to in a few years may be like buying a DOS based system to a Windows system.
I would prefer if they let physicians buy their own EMRs and not have it subsidized. It will be interesting to see how things work out over the next 3-5 years. Technology is changing rapidly. Microsoft and Google are also getting more into healthcare. EMRs available today may appear ancient compared to the new crop of EMRs coming out over the next few years. Buying an EMR today compared to in a few years may be like buying a DOS based system to a Windows system.
Sunday, November 4, 2007
New Service: Document Sharing
Check out edocr.com
This is a new service that allows users to upload various documents for sharing. You can even embed documents in your web pages as shown below. Think of it like a Youtube for documents.
This is a new service that allows users to upload various documents for sharing. You can even embed documents in your web pages as shown below. Think of it like a Youtube for documents.
Medicare Rate Reduction
This is really unfortunate. I know of several physicians that I work with who will be closing their doors to new medicare patients. Some may wrongly conclude this is just greed on the part of doctors. Its really about the physicians ability to deliver quality medical care however. Medicare patients are a very complex group of patients. Life expectancy is higher, there are new drugs to treat new conditions. These patients are frequently hospitalized and move from care setting to care setting (hospitals, nursing homes, Rehabs etc). They frequently require state-of-the art diagnostic testing. Keeping track of all these issues, dealing with long family visits, phones calls, coordinating care is all too time consuming. With decreasing resources, there is a limit to how far a physician can extend themselves.
For more information, take a look at FierceHealthIT, Physicians see expected 10 percent Medicare cut.
For more information, take a look at FierceHealthIT, Physicians see expected 10 percent Medicare cut.
Saturday, November 3, 2007
Office Open XML for Healthcare
Roberto Ruggeri posted the following on his blog:
Using Office Open XML Formats to Support Electronic Health Records Portability and Health Industry Standards
It includes sample code
Here is a description taken from the site:
Using Office Open XML Formats to Support Electronic Health Records Portability and Health Industry Standards
It includes sample code
Here is a description taken from the site:
"Empowering patients and consumers to securely exchange Electronic Health Records is a big debate in the Health industry across the globe. In this article, we discuss some techniques that use Office Open XML Formats and how to embed custom XML formats to exchange data securely. This particular scenario shows the use of Health Level Seven (HL7) Clinical Document Architecture (CDA) to represent the Electronic Health Record in an industry standard format. It also shows how to include the data in a secured document, based on Office Open XML Formats, for portability across multiple care providers."
Our healthcare costs not producing results? My take on this matter
The money we spend on healthcare in this country does not all go towards improving mortality or disease outcomes statistics. As a practicing physician, I can tell you that we spend more healthcare dollars trying to meet our patient's expectations and in practicing defensive medicine than in actually improving outcomes.
Example: Patients who present with low back many times have the expectation that they will need an MRI. Even if I'm able to convince them that an MRI is not justified in the acute stages of low back pain, if they are not better in the next few weeks, they will demand an MRI. In many cases, the doctor will go ahead and order the MRI at that point. In this low back pain case, the cost of healthcare goes up steeply after the MRI is ordered. Now will there be any improvement in any outcome measures of back pain as a result? Most likely no. Studies have repeatedly shown this to be the case. In fact, for most back pain cases, patients get better with simple, low cost conservative treatment such as back rest.
A similar case of low back pain treated in a third word country would likely have a similar outcome as in this country- the patient gets better after a few months of conservative treatment. In this country however, we will have spent money on countless office visits, MRIs, physical therapy etc, while in a third world country, the only cost would have been a single office visit. So does this mean that our healthcare system has inferior outcomes? No, its just that our healthcare users have a different set of expectations from their healthcare system than in other countries.
As far as "defensive medicine" and costs, when there's an unfortunate healthcare outcome for example, in this country it's automatically assumed in many cases that it's the fault of the healthcare provider. Remember the recent ex-Patriot coach, Charlie Weis's lawsuit? Situations like this natuarally effect the practice of medicine by our healthcare providers.
For better or worse, our healthcare dollars do not all go towards improving outcome statistics. The cost of healthcare, as well as happiness in general, is just higher in this country.
Example: Patients who present with low back many times have the expectation that they will need an MRI. Even if I'm able to convince them that an MRI is not justified in the acute stages of low back pain, if they are not better in the next few weeks, they will demand an MRI. In many cases, the doctor will go ahead and order the MRI at that point. In this low back pain case, the cost of healthcare goes up steeply after the MRI is ordered. Now will there be any improvement in any outcome measures of back pain as a result? Most likely no. Studies have repeatedly shown this to be the case. In fact, for most back pain cases, patients get better with simple, low cost conservative treatment such as back rest.
A similar case of low back pain treated in a third word country would likely have a similar outcome as in this country- the patient gets better after a few months of conservative treatment. In this country however, we will have spent money on countless office visits, MRIs, physical therapy etc, while in a third world country, the only cost would have been a single office visit. So does this mean that our healthcare system has inferior outcomes? No, its just that our healthcare users have a different set of expectations from their healthcare system than in other countries.
As far as "defensive medicine" and costs, when there's an unfortunate healthcare outcome for example, in this country it's automatically assumed in many cases that it's the fault of the healthcare provider. Remember the recent ex-Patriot coach, Charlie Weis's lawsuit? Situations like this natuarally effect the practice of medicine by our healthcare providers.
For better or worse, our healthcare dollars do not all go towards improving outcome statistics. The cost of healthcare, as well as happiness in general, is just higher in this country.
Friday, November 2, 2007
HL7 v3 sample Code from Microsoft
My complaint has always been the lack of available open source code for HL7 v3. Microsoft has been great in recent years by releasing sample .NET code such as the "Application Blocks" (see for example) and various reference architectures. They have now released code for a working sample HL7 v3 application using BizTalk. I'm not really crazy about the undue complexity in implementing HL7 v3, but I hope Microsoft can make it more practical to implement using their platforms such as BizTalk.
Go take a look at Roberto Ruggeri's blog item: Getting Started with HL7 Version 3 and BizTalk Server 2006 (R2) for more information.
Here is the link to the sample code. Here is the whitepaper on getting started with BizTalk and HL7 v3.
Go take a look at Roberto Ruggeri's blog item: Getting Started with HL7 Version 3 and BizTalk Server 2006 (R2) for more information.
Here is the link to the sample code. Here is the whitepaper on getting started with BizTalk and HL7 v3.
Thursday, November 1, 2007
TeleHealth and HealthVault ?
If you are interested in TeleHealth, read this facinating account of how Microsoft's HealthVault can serve as a "HIE Type" platform rather than point-to-point connections from device to nurse to doctor. HealthVault in essence can be a central "patient centric" application to which all data would be sent. Read on...
HealthVault Lays a Foundation to Build Scale for Telehealth
Applications
Today, telehealth applications are based on point to point
relationships: home health agency to patient; disease management company
to patient; health system to patient.
Telehealth devices and their
connectivity are similar. There is a proprietary chain of key components for a
remote patient monitoring (RPM) solution: 1) the RPM device; 2) a gateway
-- which could be mobile like the Biotronik
Cardio Messenger or static like a personal computer -- to aggregate data
from multiple devices and move data to a server-based application; and 3) the
server application that stores and manages the data in accordance with the
application, e.g., glycemic control, medication compliance, etc.
Athena Health Platform and HealthVault? Just me thinking...
Just read an article in the Health Blog on Athena Health. Athena Health as you may know just had a very successful IPO. Although they initially focused on practice management functionality- medical billing etc, they have moved into the EMR space.
The back office "practice management" function (the medical billing) is a far easier nut to crack. Most doctors are already submitting claims electronically (directly or via a billing service). The EMR piece is more of a challenge and in some ways more "art" than science.
My feeling is that Athena Health should spend their efforts more on creating an interoperable "Practice management" platform in the same way Microsoft created Healthvault as a "PHR platform" rather then a PHR application. With Microsoft's approach, PHR vendors will use HealthVault as a backend platform to perform core PHR functions. In other words, Microsoft is not trying to take over the PHR space, but rather be a part of every PHR.
By creating a "Practice Management Platform", EMR vendors may design their systems to integrate with Athena Health's practice management functionality (this is done via a set of web services). The reason I say this is because those who know EMRs best are not the same people who know practice management functionality. If I was to design an EMR (which I am doing BTW), I'd much rather integrate well with a solid Practice management system than design my own.
The back office "practice management" function (the medical billing) is a far easier nut to crack. Most doctors are already submitting claims electronically (directly or via a billing service). The EMR piece is more of a challenge and in some ways more "art" than science.
My feeling is that Athena Health should spend their efforts more on creating an interoperable "Practice management" platform in the same way Microsoft created Healthvault as a "PHR platform" rather then a PHR application. With Microsoft's approach, PHR vendors will use HealthVault as a backend platform to perform core PHR functions. In other words, Microsoft is not trying to take over the PHR space, but rather be a part of every PHR.
By creating a "Practice Management Platform", EMR vendors may design their systems to integrate with Athena Health's practice management functionality (this is done via a set of web services). The reason I say this is because those who know EMRs best are not the same people who know practice management functionality. If I was to design an EMR (which I am doing BTW), I'd much rather integrate well with a solid Practice management system than design my own.
Thin vs Thick Client and Microsoft's Smart Client
I just read a very interesting blog item on The Healthcare IT Guy, Guest Article: Rich Internet Applications for Improved Healthcare App User Experience . Since I have spent time on this issue, especially as it relates to Microsoft's Smart Client Platform, I thought I'd add my own 2 cents:
Thin vs Thick clients is always a great discussion. Microsoft has the "Smart Client" platform which is essentially a thick client UI that uses web services on the back-end to connect with the data-store. This has the benefit of allowing the "Smart Client" application to work in distributed environment, just like a typical web application.
The "rich" windows UI of the Smart Client is the advantage over a web UI. Ajax however is making web applications look more like a rich Windows-like UI. Just check out, for example, the new Yahoo mail (my personal email platform).
The Smart client distinguishes itself by allowing for an "off-line" mode, which is great in scenarios where Internet access is not always available. Installation and deployment however is the downside of the Smart Client, although it has been made easier with this platform. This is where pure web applications shine.
I wonder if Microsoft is still committed to the Smart Client now that they have another UI platform in the works, code name "Silver-Light", which will further bridge the gap between a Windows and Web UI. We'll have to just wait to see how things sort out in the end.
Thin vs Thick clients is always a great discussion. Microsoft has the "Smart Client" platform which is essentially a thick client UI that uses web services on the back-end to connect with the data-store. This has the benefit of allowing the "Smart Client" application to work in distributed environment, just like a typical web application.
The "rich" windows UI of the Smart Client is the advantage over a web UI. Ajax however is making web applications look more like a rich Windows-like UI. Just check out, for example, the new Yahoo mail (my personal email platform).
The Smart client distinguishes itself by allowing for an "off-line" mode, which is great in scenarios where Internet access is not always available. Installation and deployment however is the downside of the Smart Client, although it has been made easier with this platform. This is where pure web applications shine.
I wonder if Microsoft is still committed to the Smart Client now that they have another UI platform in the works, code name "Silver-Light", which will further bridge the gap between a Windows and Web UI. We'll have to just wait to see how things sort out in the end.
Subscribe to:
Posts (Atom)




